

Combined Hepatocellular-Cholangiocarcinoma: What the Multidisciplinary Team Should Know
- PMID: 35453938
- PMCID: PMC9026907
- DOI: 10.3390/diagnostics12040890
Combined Hepatocellular-Cholangiocarcinoma: What the Multidisciplinary Team Should Know
Abstract
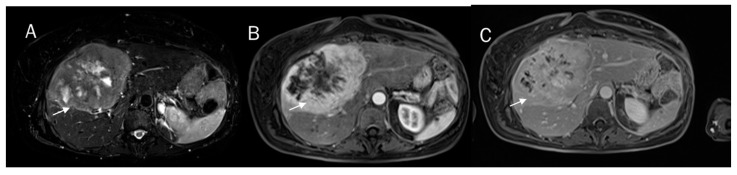
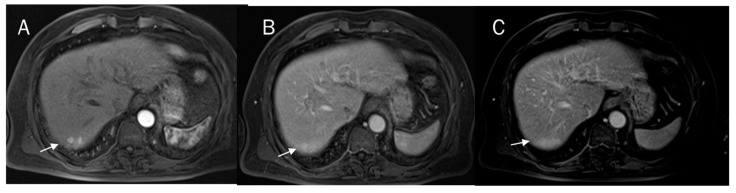
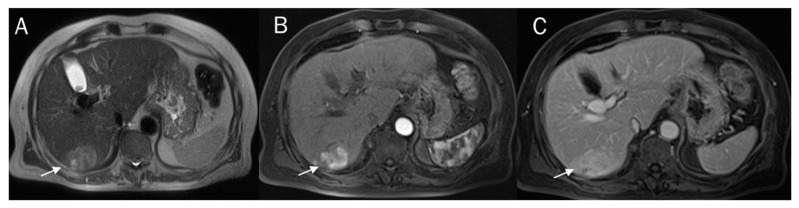
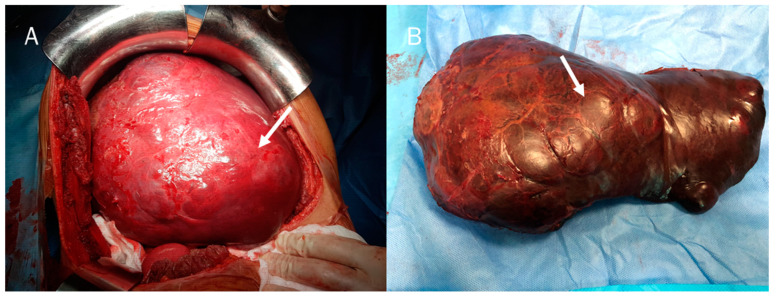
Combined hepatocellular-cholangiocarcinoma (cHCC-CCA) is a rare type of primary liver malignancy. Among the risk factors, hepatitis B and hepatitis C virus infections, cirrhosis, and male gender are widely reported. The clinical appearance of cHCC-CCA is similar to that of HCC and iCCA and it is usually silent until advanced states, causing a delay of diagnosis. Diagnosis is mainly based on histology from biopsies or surgical specimens. Correct pre-surgical diagnosis during imaging studies is very problematic and is due to the heterogeneous characteristics of the lesion in imaging, with overlapping features of HCC and CCA. The predominant histological subtype within the lesion establishes the predominant imaging findings. Therefore, in this scenario, the radiological findings characteristic of HCC show an overlap with those of CCA. Since cHCC-CCAs are prevalent in patients at high risk of HCC and there is a risk that these may mimic HCC, it is currently difficult to see a non-invasive diagnosis of HCC. Surgery is the only curative treatment of HCC-CCA. The role of liver transplantation (LT) in the treatment of cHCC-CCA remains controversial, as is the role of ablative or systemic therapies in the treatment of this tumour. These lesions still remain challenging, both in diagnosis and in the treatment phase. Therefore, a pre-treatment imaging diagnosis is essential, as well as the identification of prognostic factors that could stratify the risk of recurrence and the most adequate therapy according to patient characteristics.
Keywords: CT; LI-RADS; MRI; ablative treatment; cHCC-CCA; diagnosis; surgical resection.
Conflict of interest statement
The authors have no conflict of interest to be disclosed. The authors confirm that the article is not under consideration for publication elsewhere. Each author has participated sufficiently to take public responsibility for the manuscript content.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
