

Osteoprotegerin Is a Better Predictor for Cardiovascular and All-Cause Mortality than Vascular Calcifications in a Multicenter Cohort of Patients on Peritoneal Dialysis
- PMID: 35454141
- PMCID: PMC9025174
- DOI: 10.3390/biom12040551
Osteoprotegerin Is a Better Predictor for Cardiovascular and All-Cause Mortality than Vascular Calcifications in a Multicenter Cohort of Patients on Peritoneal Dialysis
Abstract
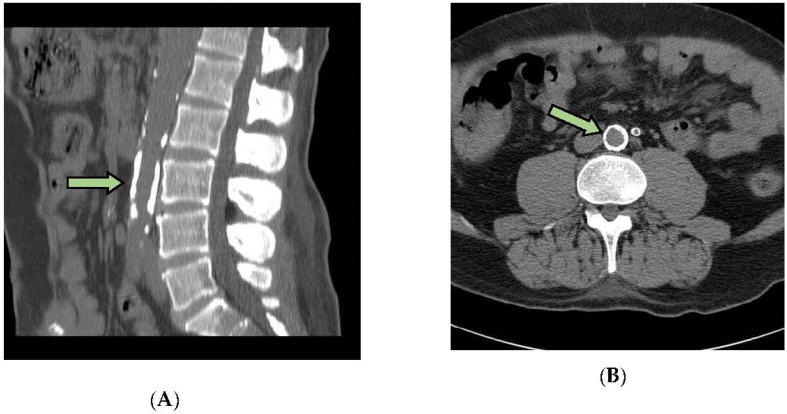
The purpose of this study was to compare vascular calcification (VC), serum osteoprotegerin (OPG) levels, and other biochemical markers to determine their value as available predictors of all-cause and cardiovascular (CV) mortality in patients on peritoneal dialysis (PD). A total of 197 patients were recruited from seven dialysis centers in Mexico City. VC was assessed with multi-slice computed tomography, measured using the calcification score (CaSc). OPG, albumin, calcium, hsC-reactive protein, phosphorous, osteocalcin, total alkaline phosphatase, and intact parathormone were also analyzed. Follow-up and mortality analyses were assessed using the Cox regression model. The mean age was 43.9 ± 12.9 years, 64% were males, and 53% were diabetics. The median OPG was 11.28 (IQR: 7.6−17.4 pmol/L), and 42% of cases had cardiovascular calcifications. The median VC was 424 (IQR:101−886). During follow-up (23 ± 7 months), there were 34 deaths, and 44% were cardiovascular in origin. In multivariable analysis, OPG was a significant predictor for all-cause (HR 1.08; p < 0.002) and CV mortality (HR 1.09; p < 0.013), and performed better than VC (HR 1.00; p < 0.62 for all-cause mortality and HR 1.00; p < 0.16 for CV mortality). For each mg/dL of albumin-corrected calcium, there was an increased risk for CV mortality, and each g/dL of albumin decreased the risk factor for all-cause mortality. OPG levels above 14.37 and 13.57 pmol/L showed the highest predictive value for all-cause and CV mortality in incident PD patients and performed better than VC.
Keywords: cardiovascular mortality; diabetes mellitus; osteoprotegerin; peritoneal dialysis; risk factor; vascular calcification.
Conflict of interest statement
The authors declare no conflict of interest.
Figures



References
-
- Foley R.N., Murray A.M., Li S., Herzog C.A., McBean A.M., Eggers P.W., Collins A.J. Chronic kidney disease and the risk for cardiovascular disease, renal replacement, and death in the United States Medicare population, 1998 to 1999. J. Am. Soc. Nephrol. JASN. 2005;16:489–495. doi: 10.1681/ASN.2004030203. - DOI - PubMed
-
- London G.M. Arteriosclerosis and arterial calcifications in chronic kidney insufficiency. Nephrol. Ther. 2005;1((Suppl. 4)):S351–S354. - PubMed
-
- Gorriz J.L., Molina P., Cerveron M.J., Vila R., Bover J., Nieto J., Barril G., Martinez-Castelao A., Fernandez E., Escudero V., et al. Vascular calcification in patients with nondialysis CKD over 3 years. Clin. J. Am. Soc. Nephrol. CJASN. 2015;10:654–666. doi: 10.2215/CJN.07450714. - DOI - PMC - PubMed
-
- Okuno S., Ishimura E., Kitatani K., Fujino Y., Kohno K., Maeno Y., Maekawa K., Yamakawa T., Imanishi Y., Inaba M., et al. Presence of abdominal aortic calcification is significantly associated with all-cause and cardiovascular mortality in maintenance hemodialysis patients. Am. J. Kidney Dis. 2007;49:417–425. doi: 10.1053/j.ajkd.2006.12.017. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
