

'Teratoid' Hepatoblastoma: An Intriguing Variant of Mixed Epithelial-Mesenchymal Hepatoblastoma
- PMID: 35455609
- PMCID: PMC9024637
- DOI: 10.3390/children9040565
'Teratoid' Hepatoblastoma: An Intriguing Variant of Mixed Epithelial-Mesenchymal Hepatoblastoma
Abstract
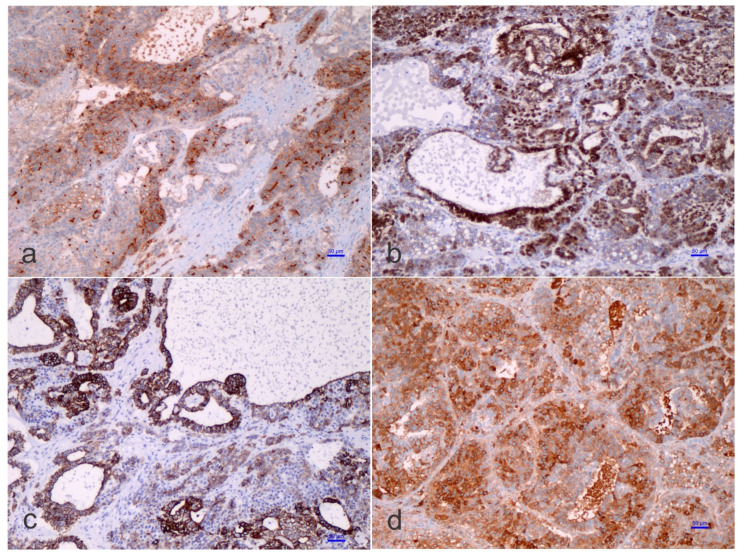
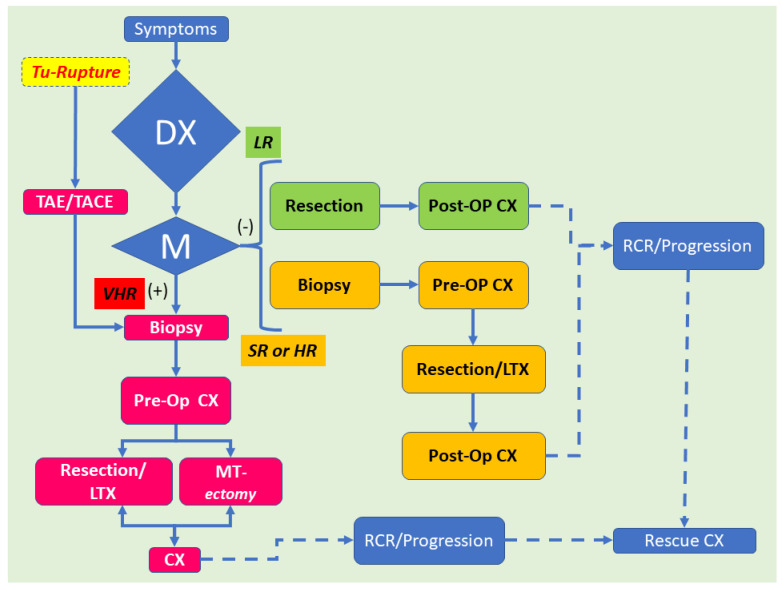
Liver neoplasms are quite rare in childhood. They often involve 6.7 cases per 10 million children aged 18 years or younger. Hepatoblastoma (HB) is the most frequent tumor, but this neoplasm's rarity points essentially to the difficulty of performing biologic studies and large-scale therapeutic trials. On the pathological ground, HB is separated into an entirely epithelial neoplasm or a mixed neoplasm with epithelial and mesenchymal components. This last category has been further subdivided into harboring teratoid features or not. The 'teratoid' HB includes a mixture of components with heterologous origin. The heterologous components include neuroectoderm, endoderm, or melanin-holding cells with or without mesenchymal components. The most important criterium for the teratoid component is neuroepithelium, melanin, and, more recently, a yolk-sac-like component and neuroendocrine components. The mesenchymal components include muscle, osteoid, and cartilage, which are most often observed mainly in 'teratoid' neoplasms. The teratoid component or mesenchymal components are diagnosed with biopsies. They appear more prominent after chemotherapy due to the response and shrinkage of epithelial elements and non- or low-responsive components of mixed HB. This review focuses on the clinical, radiological, and pathological findings of HB with teratoid features.
Keywords: cancer; liver; management; radiology.
Conflict of interest statement
The authors declare no conflict of interest.
Figures



References
-
- Guyton K.Z., Loomis D., Grosse Y., El Ghissassi F., Benbrahim-Tallaa L., Guha N., Scoccianti C., Mattock H., Straif K., International Agency for Research on Cancer Monograph Working Group Carcinogenicity of tetrachlorvinphos, parathion, malathion, diazinon, and glyphosate. Lancet Oncol. 2015;16:490–491. doi: 10.1016/S1470-2045(15)70134-8. - DOI - PubMed
-
- Guyton K.Z., Loomis D., Grosse Y., El Ghissassi F., Bouvard V., Benbrahim-Tallaa L., Guha N., Mattock H., Straif K., International Agency for Research on Cancer Monograph Working Group Carcinogenicity of pentachlorophenol and some related compounds. Lancet Oncol. 2016;17:1637–1638. doi: 10.1016/S1470-2045(16)30513-7. - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
