

Promising Effects of Digital Chest Tube Drainage System for Pulmonary Resection: A Systematic Review and Network Meta-Analysis
- PMID: 35455628
- PMCID: PMC9029690
- DOI: 10.3390/jpm12040512
Promising Effects of Digital Chest Tube Drainage System for Pulmonary Resection: A Systematic Review and Network Meta-Analysis
Abstract
Objective: The chest tube drainage system (CTDS) of choice for the pleural cavity after pulmonary resection remains controversial. This systematic review and network meta-analysis (NMA) aimed to assess the length of hospital stay, chest tube placement duration, and prolonged air leak among different types of CTDS.
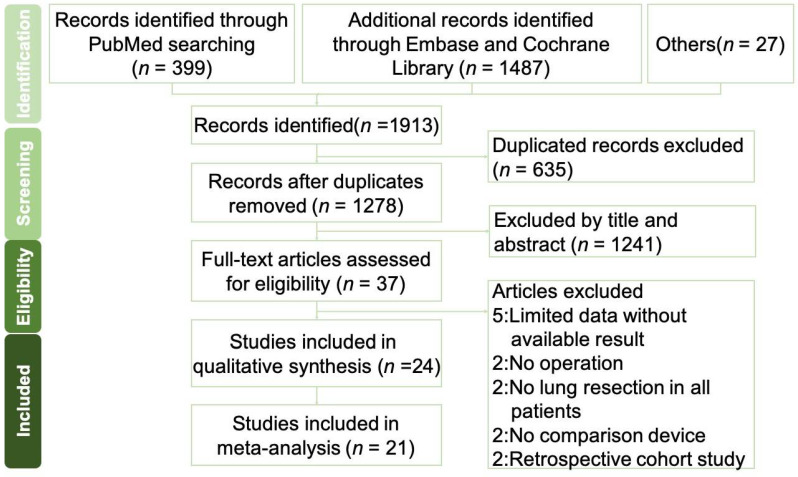
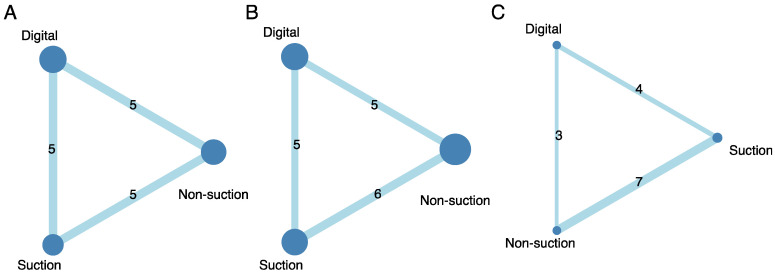
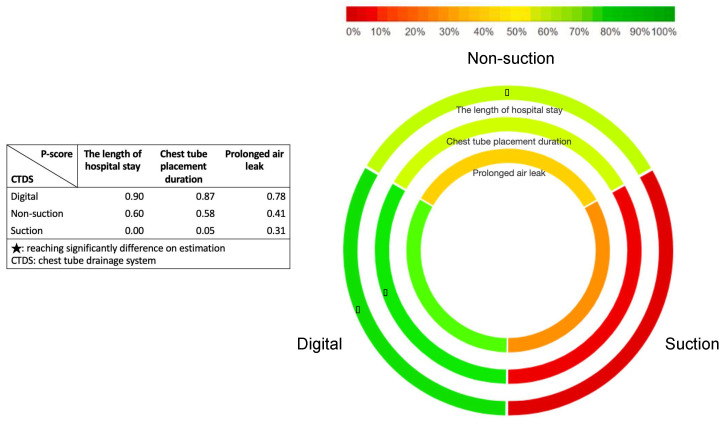
Methods: This systemic review and NMA included 21 randomized controlled trials (3399 patients) in PubMed and Embase until 1 June 2021. We performed a frequentist random effect in our NMA, and a P-score was adopted to determine the best treatment. We assessed the clinical efficacy of different CTDSs (digital/suction/non-suction) using the length of hospital stay, chest tube placement duration, and presence of prolonged air leak.
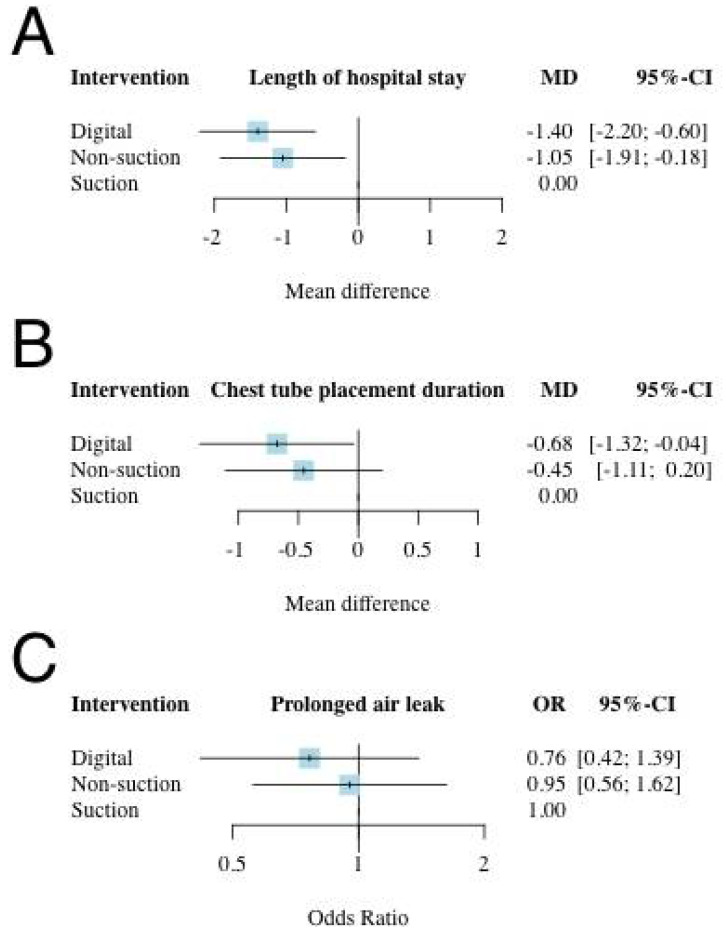
Results: Based on the NMA, digital CTDS was the most beneficial intervention for the length of hospital stay, being 1.4 days less than that of suction CTDS (mean difference (MD): -1.40; 95% confidence interval (CI): -2.20 to -0.60). Digital CTDS also had significantly reduced chest tube placement duration, being 0.68 days less than that of suction CTDSs (MD: -0.68; 95% CI: -1.32 to -0.04). Neither digital nor non-suction CTDS significantly reduced the risk of prolonged air leak.
Conclusions: Digital CTDS is associated with better outcomes than suction and non-suction CTDS for patients undergoing pulmonary resections, specifically 0.68 days shorter chest tube duration and 1.4 days shorter hospital stay than suction CTDS.
Keywords: chest tube drainage system; digital chest tube; lung resection; meta-analysis; network meta-analysis; pulmonary resection.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Batchelor T.J.P., Rasburn N.J., Abdelnour-Berchtold E., Brunelli A., Cerfolio R., Gonzalez M., Ljungqvist O., Petersen R.H., Popescu W.M., Slinger P.D., et al. Guidelines for enhanced recovery after lung surgery: Recommendations of the Enhanced Recovery After Surgery (ERAS®) Society and the European Society of Thoracic Surgeons (ESTS) Eur. J. Cardio-Thorac. Surg. 2018;55:91–115. doi: 10.1093/ejcts/ezy301. - DOI - PubMed
LinkOut - more resources
Full Text Sources
