

Endoscopic Combined Intrarenal Surgery Versus Percutaneous Nephrolithotomy for Complex Renal Stones: A Systematic Review and Meta-Analysis
- PMID: 35455648
- PMCID: PMC9028407
- DOI: 10.3390/jpm12040532
Endoscopic Combined Intrarenal Surgery Versus Percutaneous Nephrolithotomy for Complex Renal Stones: A Systematic Review and Meta-Analysis
Abstract
Background: Endoscopic combined intrarenal surgery (ECIRS) adds ureteroscopic vision to percutaneous nephrolithotomy (PCNL), which can be helpful when dealing with complex renal stones. Yet, there is still no consensus on the superiority of ECIRS. We aimed to critically analyze the available evidence of studies comparing efficacy, safety, bleeding risk, and efficiency of ECIRS and PCNL.
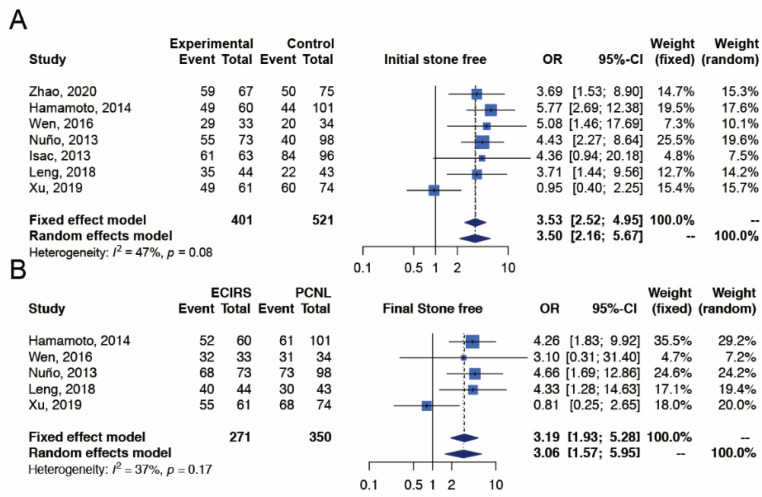
Methods: We searched for studies comparing efficacy (initial and final stone-free rate), safety (postoperative fever, overall and severe complications), efficiency (operative time and hospital stay) and bleeding risk between ECIRS and PCNL. Meta-analysis was performed.
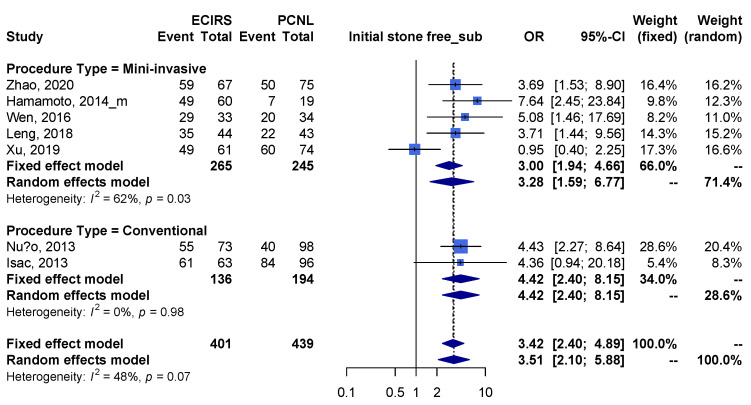
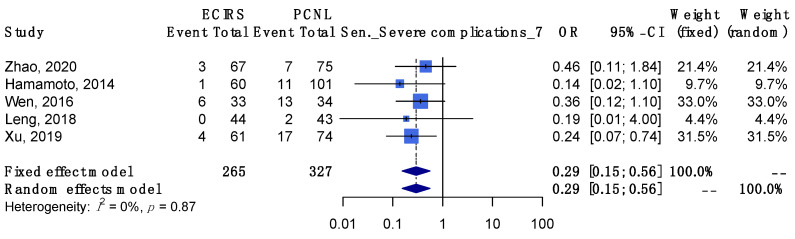
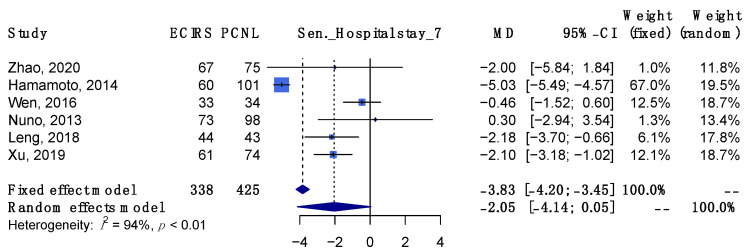
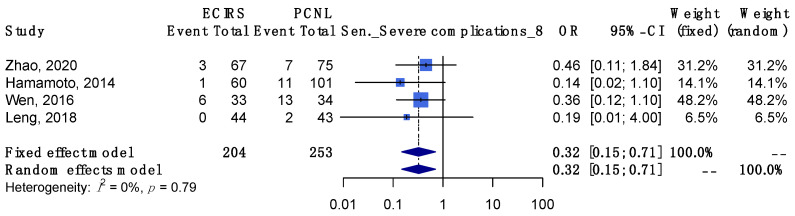
Results: Seven studies (919 patients) were identified. ECIRS provided a significantly higher initial stone-free rate, higher final stone-free rate, lower overall complications, lower severe complications, and lower rate of requiring blood transfusion. There was no difference between the two groups in terms of postoperative fever, hemoglobin drop, operative time, and hospital stay. In the subgroup analysis, both minimally invasive and conventional ECIRS were associated with a higher stone-free rate and lower complication outcomes.
Conclusions: When treating complex renal stones, ECIRS has a better stone-free rate, fewer complications, and requires fewer blood transfusions compared with PCNL. Subgroups either with minimally invasive or conventional intervention showed a consistent trend.
Keywords: complex renal stones; efficiency; endoscopic combined intrarenal surgery; percutaneous nephrolithotomy; safety; stone-free rates.
Conflict of interest statement
The authors declare no conflict of interest.
Figures




















































Similar articles
-
Endoscopic Combined Intrarenal Surgery vs Percutaneous Nephrolithotomy for Large and Complex Renal Stone: A Systematic Review and Meta-Analysis.J Endourol. 2022 Jul;36(7):865-876. doi: 10.1089/end.2021.0761. Epub 2022 Jun 24. J Endourol. 2022. PMID: 35152754
-
Comparison of mini endoscopic combined intrarenal surgery and multitract minimally invasive percutaneous nephrolithotomy specifically for kidney staghorn stones: a single-centre experience.BMC Urol. 2022 Jun 30;22(1):93. doi: 10.1186/s12894-022-01030-7. BMC Urol. 2022. PMID: 35773639 Free PMC article.
-
Is endoscopic combined intrarenal surgery ready for primetime in endourology? Outcomes from a systematic review and meta-analysis.Cent European J Urol. 2022;75(2):171-181. doi: 10.5173/ceju.2022.0049. Epub 2022 Apr 29. Cent European J Urol. 2022. PMID: 35937663 Free PMC article. Review.
-
Endoscopic combined intrarenal surgery for large calculi: simultaneous use of flexible ureteroscopy and mini-percutaneous nephrolithotomy overcomes the disadvantageous of percutaneous nephrolithotomy monotherapy.J Endourol. 2014 Jan;28(1):28-33. doi: 10.1089/end.2013.0361. Epub 2013 Oct 24. J Endourol. 2014. PMID: 23987470
-
A comparative study of endoscopic combined intrarenal surgery (ECIRS) in the galdakao-modified supine valdivia (GMSV) position and minimally invasive percutaneous nephrolithotomy for complex nephrolithiasis: a retrospective single-center study.Urolithiasis. 2021 Apr;49(2):161-166. doi: 10.1007/s00240-020-01207-5. Epub 2020 Aug 10. Urolithiasis. 2021. PMID: 32776245
Cited by
-
Endoscopic Combined Intrarenal Surgery for a Large Stone in a Rare Fused Supernumerary Kidney.Cureus. 2024 Dec 26;16(12):e76438. doi: 10.7759/cureus.76438. eCollection 2024 Dec. Cureus. 2024. PMID: 39867073 Free PMC article.
-
Percutaneous Nephrolithotomy Combined Antegrade Flexible Ureteroscope for Complete Staghorn Stones: A Case Report of a New Concept of Stone Surgery.Medicina (Kaunas). 2022 Dec 23;59(1):35. doi: 10.3390/medicina59010035. Medicina (Kaunas). 2022. PMID: 36676659 Free PMC article.
-
Antegrade flexible ureteroscopy-assisted percutaneous nephrolithotomy for staghorn calculi: a prospective randomized controlled study.Urolithiasis. 2024 Feb 10;52(1):33. doi: 10.1007/s00240-024-01528-9. Urolithiasis. 2024. PMID: 38340170 Free PMC article. Clinical Trial.
-
Endoscopic combined intrarenal surgery for successful removal of an encrusted ureteral stent and multiple renal stones in solitary kidney: A case report.Int J Surg Case Rep. 2024 Feb;115:109324. doi: 10.1016/j.ijscr.2024.109324. Epub 2024 Feb 1. Int J Surg Case Rep. 2024. PMID: 38308996 Free PMC article.
-
Current role of endoscopic combined intrarenal surgery in the management of renal stones: A scoping review.Indian J Urol. 2023 Oct-Dec;39(4):274-284. doi: 10.4103/iju.iju_249_23. Epub 2023 Sep 29. Indian J Urol. 2023. PMID: 38077207 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
Medical
