

Personalized Immunotherapies for Type 1 Diabetes: Who, What, When, and How?
- PMID: 35455658
- PMCID: PMC9031881
- DOI: 10.3390/jpm12040542
Personalized Immunotherapies for Type 1 Diabetes: Who, What, When, and How?
Abstract
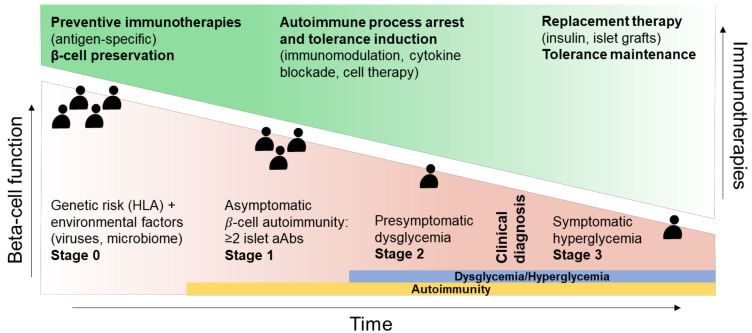
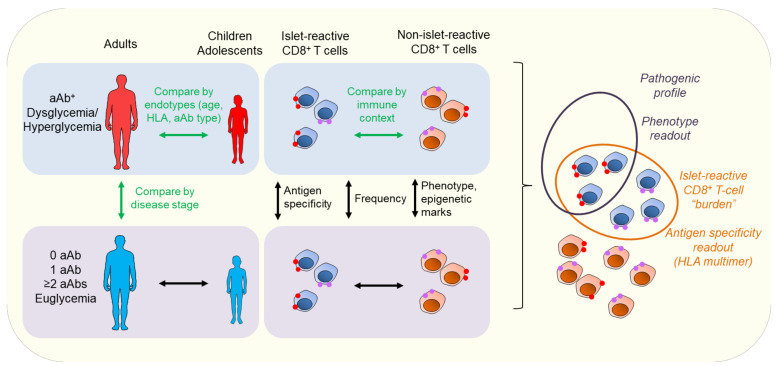
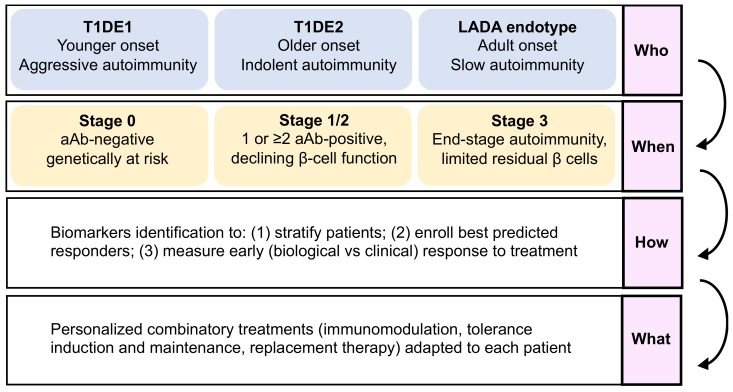
Our understanding of the immunopathological features of type 1 diabetes (T1D) has greatly improved over the past two decades and has shed light on disease heterogeneity dictated by multiple immune, metabolic, and clinical parameters. This may explain the limited effects of immunotherapies tested so far to durably revert or prevent T1D, for which life-long insulin replacement remains the only therapeutic option. In the era of omics and precision medicine, offering personalized treatment could contribute to turning this tide. Here, we discuss how to structure the selection of the right patient at the right time for the right treatment. This individualized therapeutic approach involves enrolling patients at a defined disease stage depending on the target and mode of action of the selected drug, and better stratifying patients based on their T1D endotype, reflecting intrinsic disease aggressiveness and immune context. To this end, biomarker screening will be critical, not only to help stratify patients and disease stage, but also to select the best predicted responders ahead of treatment and at early time points during clinical trials. This strategy could contribute to increase therapeutic efficacy, notably through the selection of drugs with complementary effects, and to further develop precision multi-hit medicine.
Keywords: autoantigens; autoimmunity; biomarkers; endotypes; immune tolerance; immunotherapy; personalized medicine; type 1 diabetes.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Uncovering Pathways to Personalized Therapies in Type 1 Diabetes.Diabetes. 2021 Apr;70(4):831-841. doi: 10.2337/db20-1185. Diabetes. 2021. PMID: 33741606 Free PMC article. Review.
-
A century later, still fighting back: antigen-specific immunotherapies for type 1 diabetes.Immunol Cell Biol. 2021 May;99(5):461-474. doi: 10.1111/imcb.12439. Epub 2021 Feb 11. Immunol Cell Biol. 2021. PMID: 33483995 Review.
-
A multi-omics integration approach relying on circulating factors does not discern subtypes of childhood type 1 diabetes.Commun Med (Lond). 2025 May 27;5(1):201. doi: 10.1038/s43856-025-00922-7. Commun Med (Lond). 2025. PMID: 40425874 Free PMC article.
-
Immune Checkpoint Molecules, Personalized Immunotherapy, and Autoimmune Diabetes.Trends Mol Med. 2018 Nov;24(11):931-941. doi: 10.1016/j.molmed.2018.08.005. Epub 2018 Sep 17. Trends Mol Med. 2018. PMID: 30236470 Review.
-
Antigen-based immune modulation therapy for type 1 diabetes: the era of precision medicine.Lancet Diabetes Endocrinol. 2019 Jan;7(1):65-74. doi: 10.1016/S2213-8587(18)30109-8. Epub 2018 Oct 24. Lancet Diabetes Endocrinol. 2019. PMID: 30528100 Review.
Cited by
-
A Plasma miR-193b-365 Signature Combined With Age and Glycemic Status Predicts Response to Lactococcus lactis-Based Antigen-Specific Immunotherapy in New-Onset Type 1 Diabetes.Diabetes. 2023 Oct 1;72(10):1470-1482. doi: 10.2337/db22-0852. Diabetes. 2023. PMID: 37494666 Free PMC article.
-
Phenotypic Spectrum at Diagnosis of Age-Related Endotypes of Type 1 Diabetes Mellitus: A Cross-Sectional Study in China.J Diabetes. 2025 Jun;17(6):e70111. doi: 10.1111/1753-0407.70111. J Diabetes. 2025. PMID: 40501403 Free PMC article.
-
Epitope-based precision immunotherapy of Type 1 diabetes.Hum Vaccin Immunother. 2023 Dec 31;19(1):2154098. doi: 10.1080/21645515.2022.2154098. Epub 2023 Jan 19. Hum Vaccin Immunother. 2023. PMID: 36656048 Free PMC article.
-
A set of circulating microRNAs belonging to the 14q32 chromosome locus identifies two subgroups of individuals with recent-onset type 1 diabetes.Cell Rep Med. 2024 Jun 18;5(6):101591. doi: 10.1016/j.xcrm.2024.101591. Epub 2024 Jun 4. Cell Rep Med. 2024. PMID: 38838677 Free PMC article.
-
Leveraging artificial intelligence and machine learning to accelerate discovery of disease-modifying therapies in type 1 diabetes.Diabetologia. 2025 Mar;68(3):477-494. doi: 10.1007/s00125-024-06339-6. Epub 2024 Dec 19. Diabetologia. 2025. PMID: 39694914 Free PMC article. Review.
References
-
- Pugliese A., Zeller M., Fernandez A., Zalcberg L.J., Bartlett R.J., Ricordi C., Pietropaolo M., Eisenbarth G.S., Bennett S.T., Patel D.D. The Insulin Gene Is Transcribed in the Human Thymus and Transcription Levels Correlated with Allelic Variation at the INS VNTR-IDDM2 Susceptibility Locus for Type 1 Diabetes. Nat. Genet. 1997;15:293–297. doi: 10.1038/ng0397-293. - DOI - PubMed
Publication types
Grants and funding
- ANR-17-CE17-0004/Agence Nationale de la Recherche
- ANR-19-CE15-0014-01/Agence Nationale de la Recherche
- EFSD/JDRF/Lilly Programme 2019/European Foundation for the Study of Diabetes
- EQU20193007831/Fondation pour la Recherche Médicale
- 115797 and 945268 (INNODIA and INNODIA HARVEST)/Innovative Medicines Initiative
LinkOut - more resources
Full Text Sources
Miscellaneous
