

Rank-Rankl-Opg Axis in Multiple Sclerosis: The Contribution of Placenta
- PMID: 35456036
- PMCID: PMC9031903
- DOI: 10.3390/cells11081357
Rank-Rankl-Opg Axis in Multiple Sclerosis: The Contribution of Placenta
Abstract
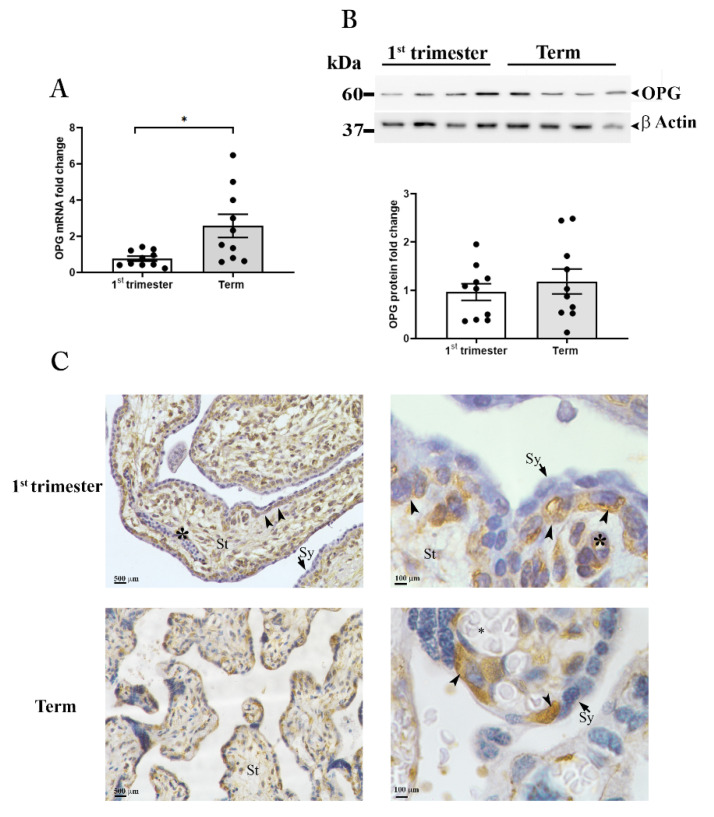
Women with multiple sclerosis (MS) can safely become pregnant and give birth, with no side effects or impediments. Pregnancy is generally accepted as a period of well-being in which relapses have a softer evolution, particularly in the third trimester. Herein, we hypothesized that the placenta, via its "secretome", could contribute to the recognized beneficial effects of pregnancy on MS activity. We focused on a well-known receptor/ligand/decoy receptor system, such as the one composed by the receptor activator of nuclear factor-kB (RANK), its ligand (RANKL), and the decoy receptor osteoprotegerin (OPG), which have never been investigated in an integrated way in MS, pregnancy, and placenta. We reported that pregnancy at the term of gestation influences the balance between circulating RANKL and its endogenous inhibitor OPG in MS women. We demonstrated that the placenta at term is an invaluable source of homodimeric OPG. By functional studies on astrocytes, we showed that placental OPG suppresses the mRNA expression of the CCL20, a chemokine responsible for Th17 cell recruitment. We propose placental OPG as a crucial molecule for the recognized beneficial effect of late pregnancy on MS and its potential utility for the development of new and more effective therapeutic approaches.
Keywords: autoimmune diseases; osteoprotegerin; placenta; pregnancy.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures




References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
