

Sex Differences in Cardiovascular Prevention in Type 2: Diabetes in a Real-World Practice Database
- PMID: 35456292
- PMCID: PMC9032335
- DOI: 10.3390/jcm11082196
Sex Differences in Cardiovascular Prevention in Type 2: Diabetes in a Real-World Practice Database
Erratum in
-
Correction: Ramírez-Morros et al. Sex Differences in Cardiovascular Prevention in Type 2: Diabetes in a Real-World Practice Database. J. Clin. Med. 2022, 11, 2196.J Clin Med. 2022 Aug 2;11(15):4492. doi: 10.3390/jcm11154492. J Clin Med. 2022. PMID: 35956255 Free PMC article.
Abstract
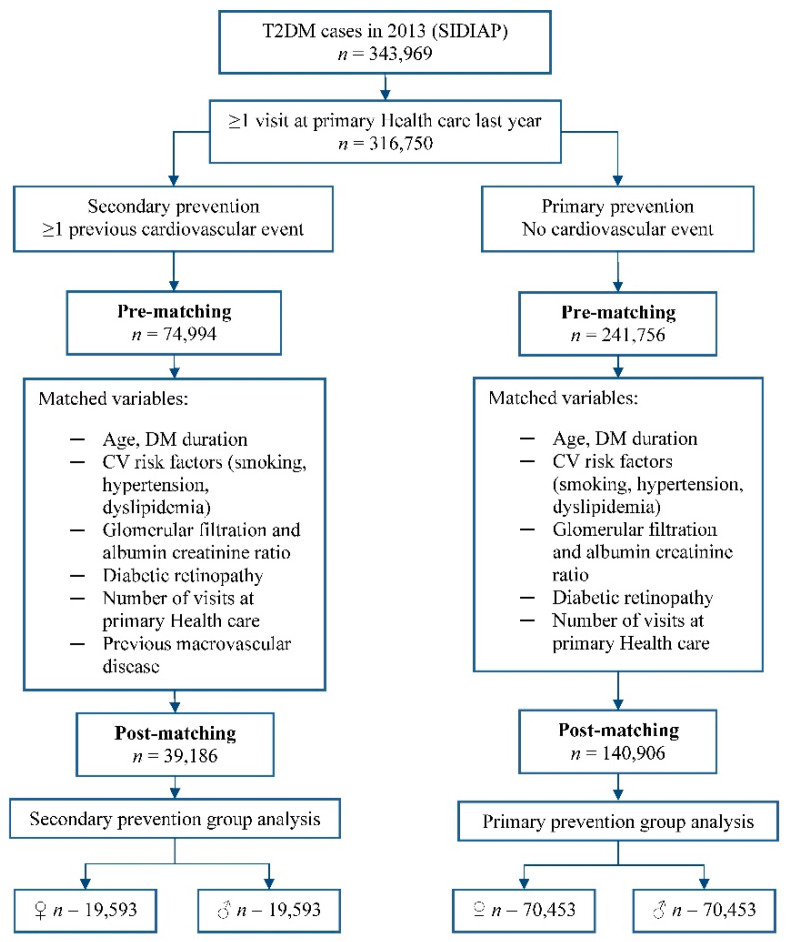
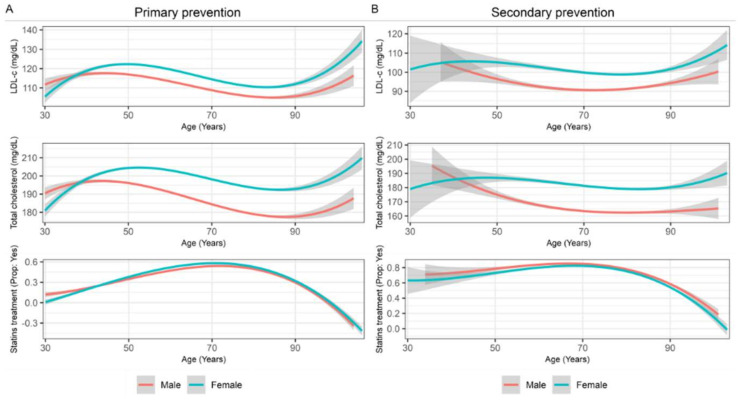
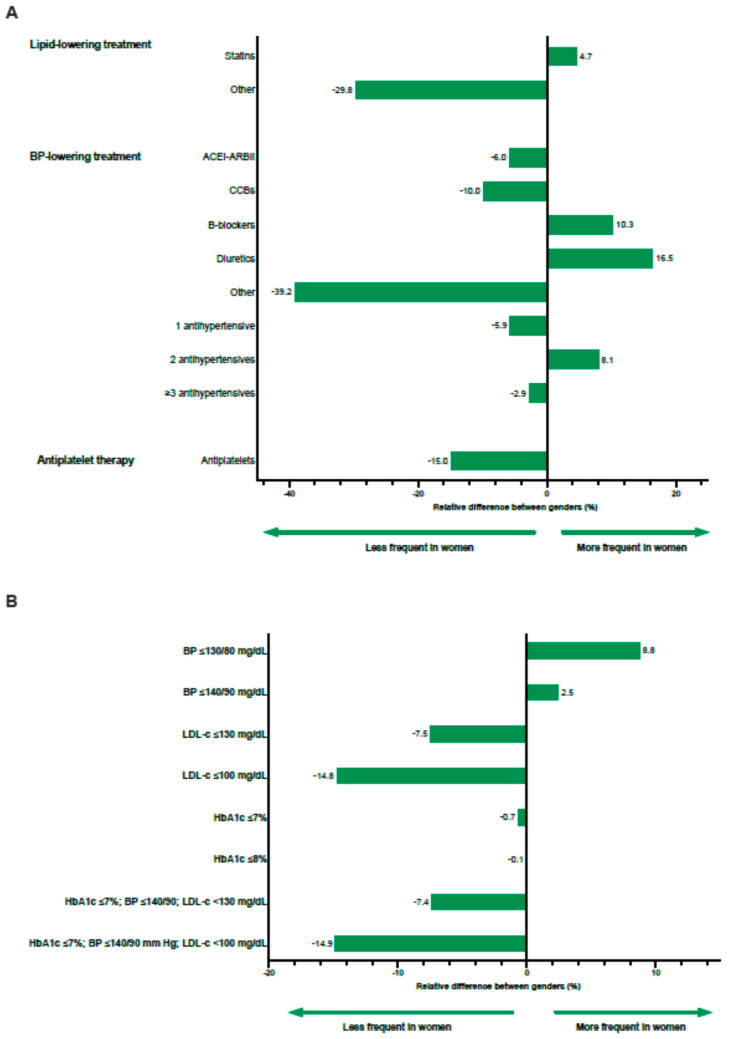
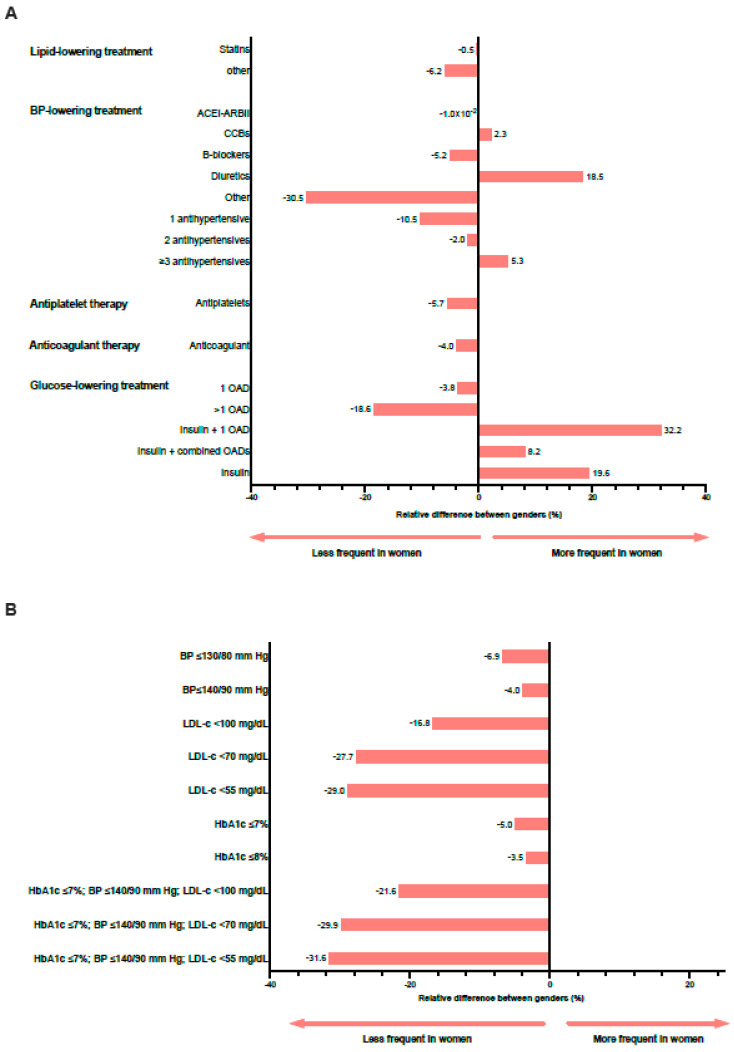
Women with type 2 diabetes mellitus (T2DM) have a 40% excess risk of cardiovascular diseases (CVD) compared to men due to the interaction between sex and gender factors in the development, risk, and outcomes of the disease. Our aim was to assess differences between women and men with T2DM in the management and degree of control of cardiovascular risk factors (CVRF). This was a matched cross-sectional study including 140,906 T2DM subjects without previous CVD and 39,186 T2DM subjects with prior CVD obtained from the System for the Development of Research in Primary Care (SIDIAP) database. The absolute and relative differences between means or proportions were calculated to assess sex differences. T2DM women without previous CVD showed higher levels of total cholesterol (12.13 mg/dL (0.31 mmol/L); 95% CI = 11.9−12.4) and low-density lipoprotein cholesterol (LDL-c; 5.50 mg/dL (0.14 mmol/L); 95% CI = 5.3−5.7) than men. The recommended LDL-c target was less frequently achieved by women as it was the simultaneous control of different CVRF. In secondary prevention, women showed higher levels of total cholesterol (16.89 mg/dL (0.44 mmol/L); 95% CI = 16.5−17.3), higher levels of LDL-c (8.42 mg/dL (0.22 mmol/L); 95% CI = 8.1−8.8), and higher levels of triglycerides (11.34 mg/dL (0.13 mmol/L); 95% CI = 10.3−12.4) despite similar rates of statin prescription. Recommended targets were less often achieved by women, especially LDL-c < 100 mg/dL (2.59 mmol/L). The composite control was 22% less frequent in women than men. In conclusion, there were substantial sex differences in CVRF management of people with diabetes, with women less likely than men to be on LDL-c target, mainly those in secondary prevention. This could be related to the treatment gap between genders.
Keywords: cardiovascular diseases; diabetes mellitus; gender; risk factors; type 2.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- International Diabetes Federation (IDF) IDF Diabetes Atlas: Ninth Edition 2019. [(accessed on 2 March 2020)]. Available online: https://www.diabetesatlas.org.
LinkOut - more resources
Full Text Sources
Miscellaneous
