

Trends in the Prevalence of Cardiometabolic Multimorbidity in the United States, 1999-2018
- PMID: 35457593
- PMCID: PMC9027860
- DOI: 10.3390/ijerph19084726
Trends in the Prevalence of Cardiometabolic Multimorbidity in the United States, 1999-2018
Abstract
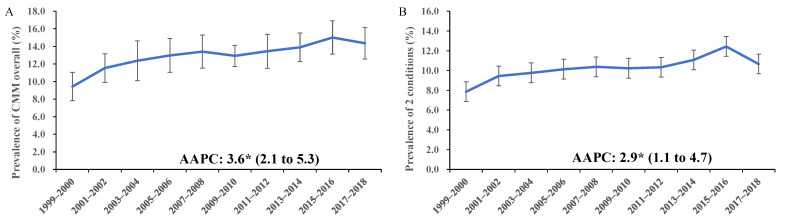
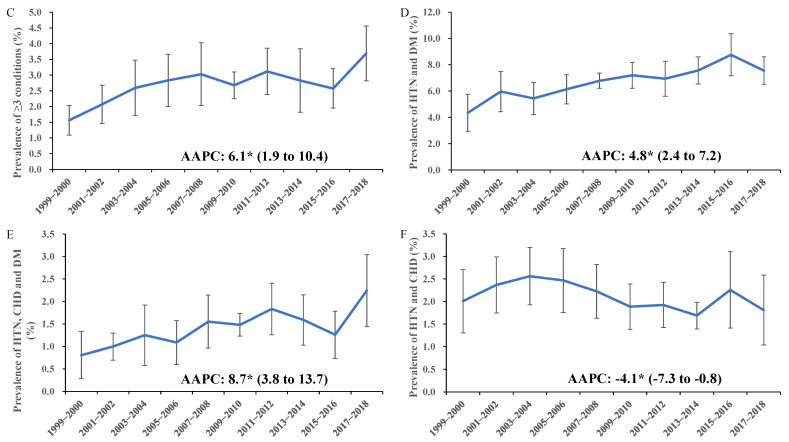
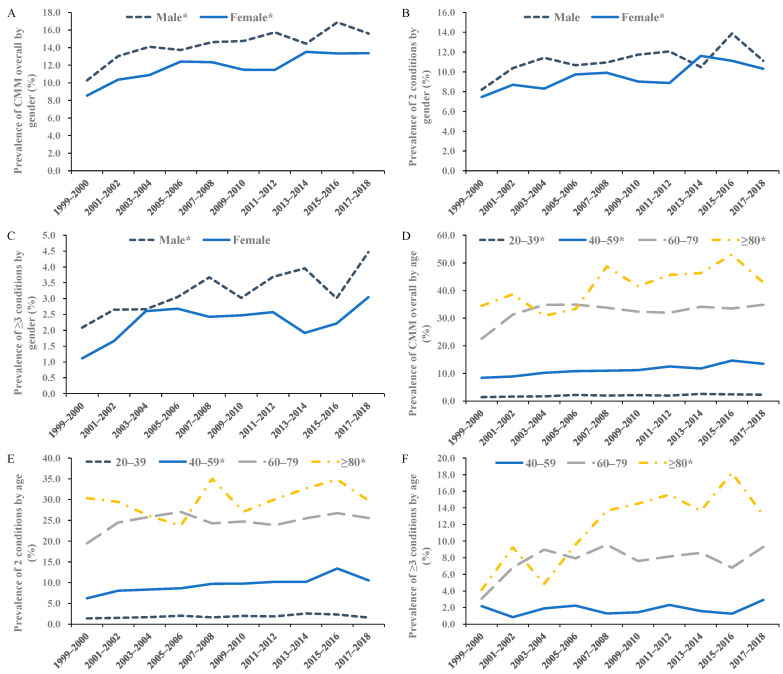
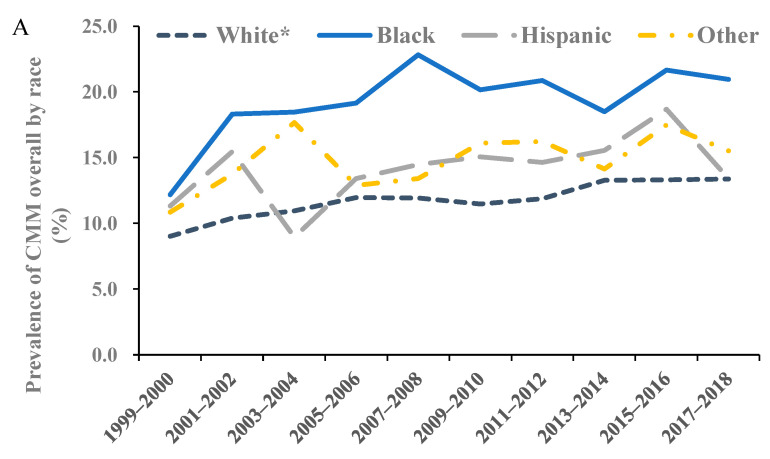
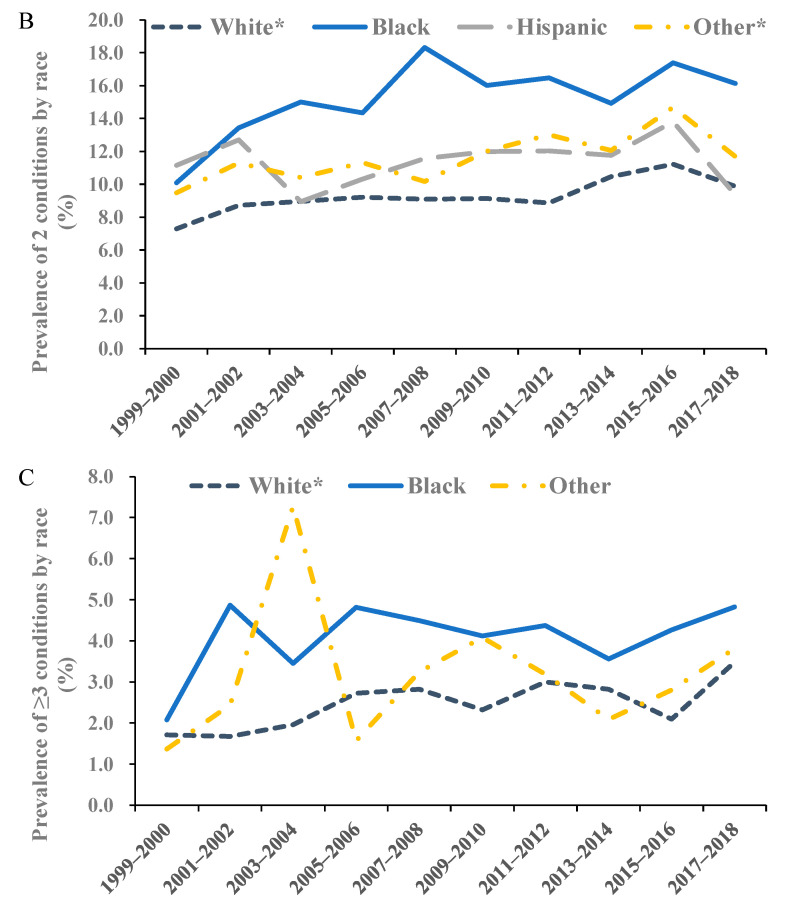
Cardiometabolic multimorbidity (co-existence of ≥1 cardiometabolic diseases) is increasingly common, while its prevalence in the U.S. is unknown. We utilized data from 10 National Health and Nutrition Examination Survey (NHANES) two-year cycles in U.S. adults from 1999 to 2018. We reported the age-standardized prevalence of cardiometabolic multimorbidity in 2017-2018 and analyzed their trends during 1999-2018 with joinpoint regression models. Stratified analyses were performed according to gender, age, and race/ethnicity. In 2017-2018, the prevalence of cardiometabolic multimorbidity was 14.4% in the U.S., and it was higher among male, older, and non-Hispanic Black people. The three most common patterns were hypertension and diabetes (7.5%); hypertension, diabetes, and CHD (2.2%); and hypertension and CHD (1.8%). During 1999-2018, the prevalence of cardiometabolic multimorbidity in U.S. adults increased significantly, with an averaged two-year cycle percentage change (AAPC) of 3.6 (95% CI: 2.1 to 5.3). The increasing trend was significant for both genders, most age groups except for 60-79 years, and non-Hispanic White people. For common patterns, the trend was increasing for hypertension and diabetes and hypertension, diabetes, and CHD, while it was decreasing for hypertension and CHD. Our findings provide evidence that cardiometabolic multimorbidity has risen as an austere issue of public health in the U.S.
Keywords: NHANES; cardiometabolic disease; epidemiology; multimorbidity.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Lyall D.M., Celis-Morales C.A., Anderson J., Gill J.M., Mackay D.F., McIntosh A.M., Smith D.J., Deary I.J., Sattar N., Pell J.P. Associations between single and multiple cardiometabolic diseases and cognitive abilities in 474 129 UK Biobank participants. Eur. Heart J. 2017;38:577–583. doi: 10.1093/eurheartj/ehw528. - DOI - PMC - PubMed
-
- Huang Z.T., Luo Y., Han L., Wang K., Yao S.S., Su H.X., Chen S., Cao G.Y., De Fries C.M., Chen Z.S., et al. Patterns of cardiometabolic multimorbidity and the risk of depressive symptoms in a longitudinal cohort of middle-aged and older Chinese. J. Affect. Disord. 2022;301:1–7. doi: 10.1016/j.jad.2022.01.030. - DOI - PubMed
-
- Maddaloni E., D’Onofrio L., Alessandri F., Mignogna C., Leto G., Pascarella G., Mezzaroma I., Lichtner M., Pozzilli P., Agro F.E., et al. Cardiometabolic multimorbidity is associated with a worse Covid-19 prognosis than individual cardiometabolic risk factors: A multicentre retrospective study (CoViDiab II) Cardiovasc. Diabetol. 2020;19:164. doi: 10.1186/s12933-020-01140-2. - DOI - PMC - PubMed
-
- McQueenie R., Foster H.M.E., Jani B.D., Katikireddi S.V., Sattar N., Pell J.P., Ho F.K., Niedzwiedz C.L., Hastie C.E., Anderson J., et al. Multimorbidity, polypharmacy, and COVID-19 infection within the UK Biobank cohort. PLoS ONE. 2020;15:e0238091. doi: 10.1371/journal.pone.0238091. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
