

Palliative care in Uganda: quantitative descriptive study of key palliative care indicators 2018-2020
- PMID: 35459171
- PMCID: PMC9023726
- DOI: 10.1186/s12904-022-00930-7
Palliative care in Uganda: quantitative descriptive study of key palliative care indicators 2018-2020
Abstract
Background: The first and most recent nationwide audit of palliative care services in Uganda was conducted in 2009. Since then, Uganda has made great strides in palliative care development, including policy, education, and services implementation. This study provides an overview of the availability of palliative care services in the country and the challenges and gaps in Uganda prior to the global COVID-19 pandemic. This lays the foundation for better understanding the challenges and changes needed to support palliative care development and access in the wake of the pandemic.
Methods: We conducted a descriptive quantitative study of secondary data on nationwide morphine distribution, collated a list of accredited facilities, and analyzed key palliative care indicators collected through the mHealth surveillance project present at a subset of accredited facilities. Descriptive statistical analysis involved non-parametric tests using SPSS, mapping geographical distribution of available palliative care services using Geographic Information Systems software, and identification of challenges from the subset of accredited facilities.
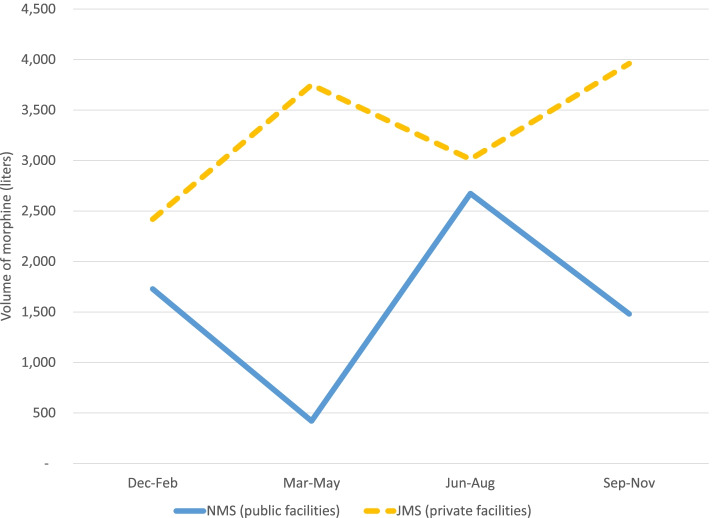
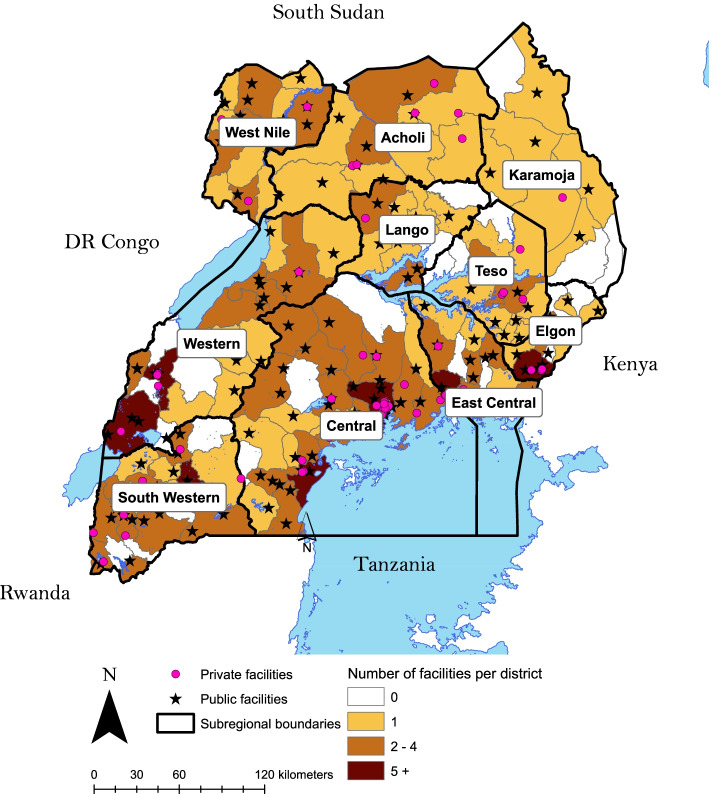
Results: There were 226 accredited palliative care facilities across Uganda's 135 districts in 2020. Thirty districts lacked any accredited palliative care facility. The estimated population coverage was 88.5%. The majority (68.1%) of accredited facilities were public, and private facilities received slightly more pain-relieving morphine. There was an alternating trend in the volumes of morphine delivered to public and private facilities. More than a third of the patients were diagnosed with non-communicable diseases, highlighting their significance alongside cancer and HIV/AIDS as conditions requiring palliative care. Palliative care accredited facilities offered six types of services: outreach, home visits, psychosocial, legal, bereavement, and spiritual support, but only for an average of 7 months a year due to lack of facilitation and transportation.
Conclusion: Palliative care in Uganda developed in quality, volume, and geographic coverage since 2009. The shift in palliative care patients' primary diagnosis from HIV/AIDS to non-communicable diseases marks an important epidemiologic transition. Although accredited facilities are present in most administrative districts, more research is needed to evaluate the actual accessibility of these services. The existing services, both private and public, are limited by the amount of pain-relieving morphine, financial and transport resources. More quality data collected on key palliative care indicators is needed into geographical accessibility of palliative care services, morphine availability trends, and patient diagnoses in order to improve the provision of palliative care in Uganda.
Keywords: Morphine; Palliative care; Uganda; mHealth.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Connor SR. Global atlas of palliative care. London: The Worldwide Hospice Palliative Care Alliance; 2020.
-
- Knaul FM, Farmer PE, Krakauer EL, De Lima L, Bhadelia A, Jiang Kwete X, et al. Alleviating the access abyss in palliative care and pain relief-an imperative of universal health coverage: the lancet commission report. Lancet. 2018;391(10128):1391–1454. doi: 10.1016/S0140-6736(17)32513-8. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
