

Screening for Social Risk at Federally Qualified Health Centers: A National Study
- PMID: 35459451
- PMCID: PMC9035213
- DOI: 10.1016/j.amepre.2021.11.008
Screening for Social Risk at Federally Qualified Health Centers: A National Study
Abstract
Introduction: Federally Qualified Health Centers serve 29.8 million low-income patients across the U.S., many of whom have unaddressed social risks. In 2019, for the first time, data on social risk screening capabilities were collected from every U.S. Federally Qualified Health Center. The objectives of this study were to describe the national rates of social risk screening capabilities across Federally Qualified Health Centers, identify organizational predictors of screening, and assess between-state heterogeneity.
Methods: Using a 100% sample of U.S. Federally Qualified Health Centers (N=1,384, representing 29.8 million patients) from the 2019 Uniform Data System, the primary outcome was whether a Federally Qualified Health Center collected data on patients' social risk factors (yes/no). Summary statistics on the rates of social risk screening capabilities were generated in aggregate and by state. Linear probability models were then used to estimate the relationship between the probability of social risk screening and 7 key Federally Qualified Health Center characteristics (e.g., Federally Qualified Health Center size, Medicaid MCO contract, Medicaid accountable care organization presence). Data were analyzed in 2020‒2021.
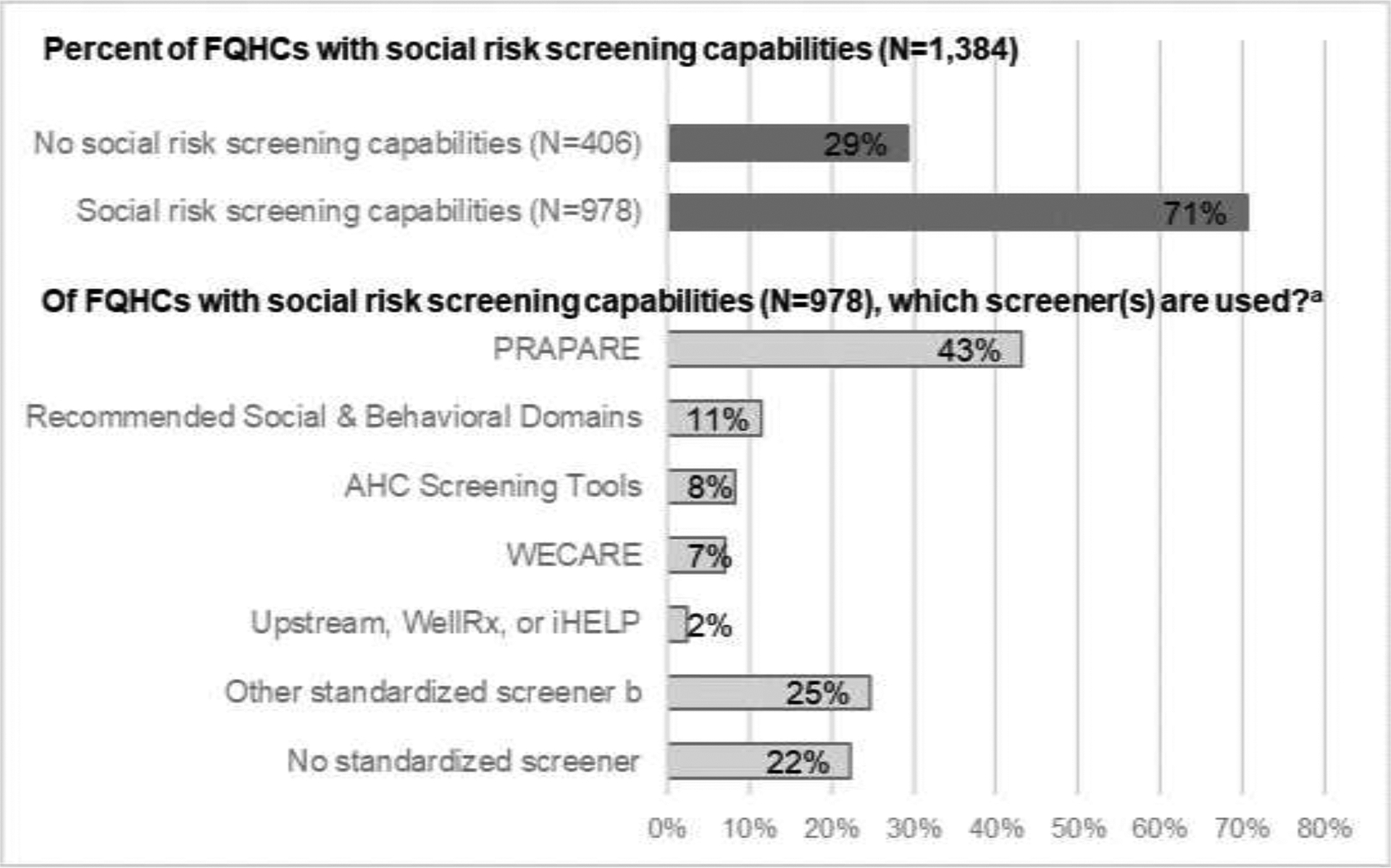
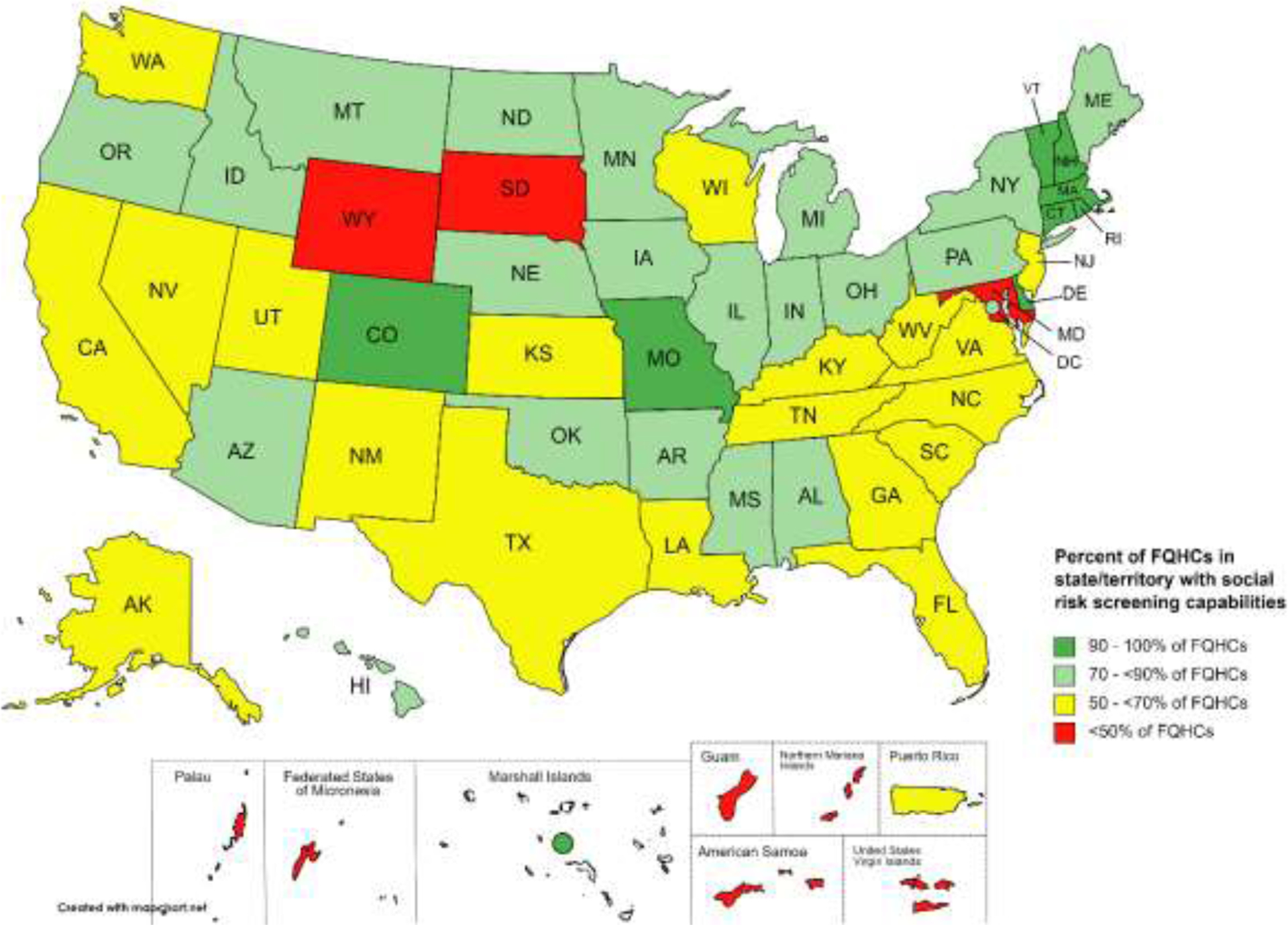
Results: Most (71%) Federally Qualified Health Centers collected social risk data, with a between-state variation. The most common screener was the Protocol for Responding to and Assessing Patients' Assets Risks and Experiences (43% of Federally Qualified Health Centers that screened), whereas 22% collected social risk data using a nonstandardized screener. After adjusting for other characteristics, Federally Qualified Health Centers with social risk screening capabilities served more total patients, were more likely to be located in a state with a Medicaid accountable care organization, and were less likely to have an MCO contract.
Conclusions: There has been widespread adoption of social risk screening tools across U.S. Federally Qualified Health Centers, but between-state disparities exist. Targeting social risk screening resources to smaller Federally Qualified Health Centers may increase the adoption of screening tools.
Copyright © 2021 American Journal of Preventive Medicine. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Health Center Program: Impact and Growth. Bureau of Primary Health Care. https://bphc.hrsa.gov/about/healthcenterprogram/index.html. Published August 20, 2018. Accessed September 24, 2020.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
