

Intracervical insemination versus intrauterine insemination with cryopreserved donor sperm in the natural cycle: a randomized controlled trial
- PMID: 35459949
- PMCID: PMC9789751
- DOI: 10.1093/humrep/deac071
Intracervical insemination versus intrauterine insemination with cryopreserved donor sperm in the natural cycle: a randomized controlled trial
Abstract
Study question: Is intracervical insemination (ICI) non-inferior to IUI with cryopreserved donor sperm in the natural cycle in terms of live birth?
Summary answer: ICI with cryopreserved donor sperm in the natural cycle was inferior to IUI in terms of live birth.
What is known already: Both ICI and IUI in the natural cycle are performed as first-line treatments in women who are eligible for donor sperm treatment. High-quality data on the effectiveness of ICI versus IUI with cryopreserved donor sperm in the natural cycle in terms of live birth is lacking.
Study design, size, duration: We performed an open-label multicentre randomized non-inferiority trial in the Netherlands and Belgium.
Participants/materials, setting, methods: We randomly allocated women who were eligible for donor sperm treatment with cryopreserved donor semen to six cycles of ICI in the natural cycle or six cycles of IUI in the natural cycle. The primary outcome was conception within 8 months after randomization leading to a live birth. Secondary outcomes were ongoing pregnancy, multiple pregnancy, clinical pregnancy, miscarriage and time to conception leading to live birth. We calculated relative risks (RRs) and risk differences (RDs) with 95% CI. Non-inferiority would be shown if the lower limit of the 95% RD CI was <-12%.
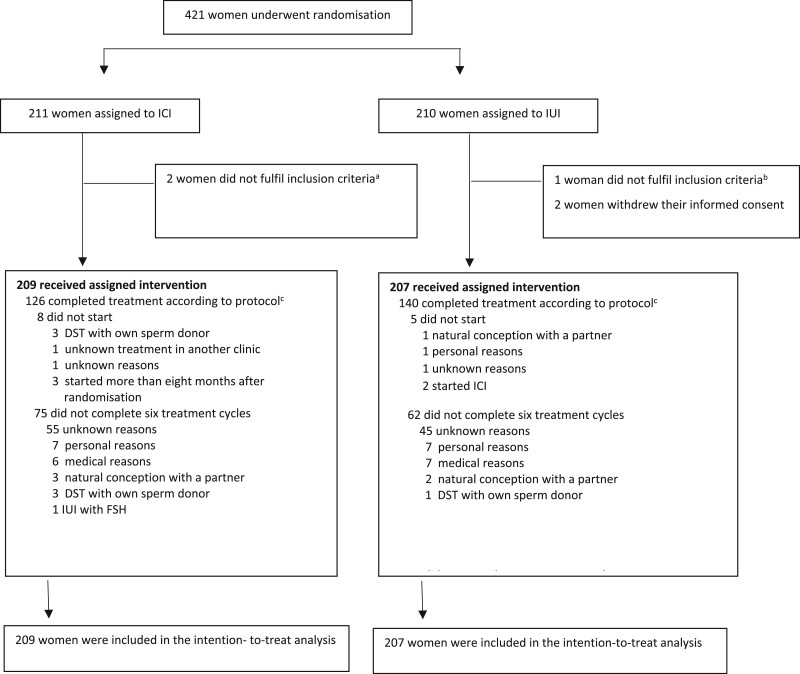
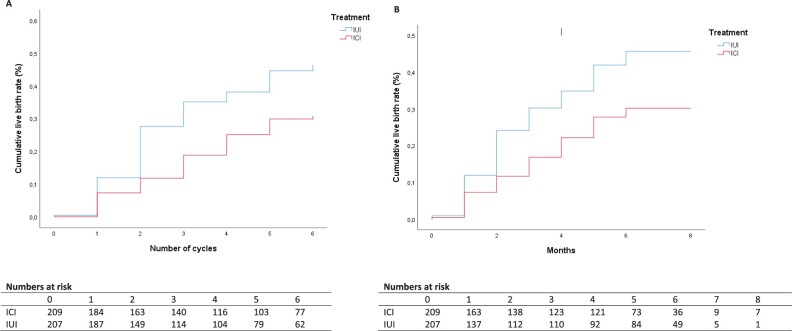
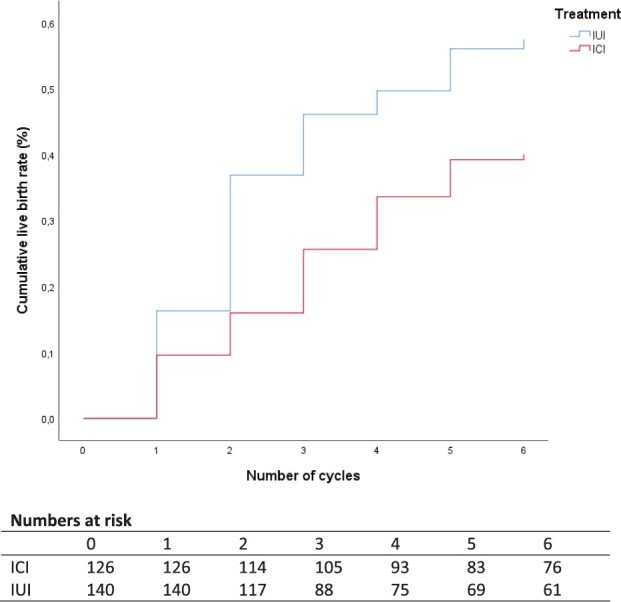
Main results and the role of chance: Between June 2014 and February 2019, we included 421 women, of whom 211 women were randomly allocated to ICI and 210 to IUI. Of the 211 women allocated to ICI, 2 women were excluded, 126 women completed treatment according to protocol and 75 women did not complete 6 treatment cycles. Of the 210 women allocated to IUI, 3 women were excluded, 140 women completed treatment according to protocol and 62 women did not complete 6 treatment cycles. Mean female age was 34 years (SD ±4) in both interventions. Conception leading to live birth occurred in 51 women (24%) allocated to ICI and in 81 women (39%) allocated to IUI (RR 0.63, 95% CI: 0.47 to 0.84). This corresponds to an absolute RD of -15%; 95% CI: -24% to -6.9%, suggesting inferiority of ICI. ICI also resulted in a lower live birth rate over time (hazard ratio 0.58, 95% CI: 0.41-0.82). Our per-protocol analysis showed that, within the 8 months treatment horizon, 48 women (38%) had live births after ICI and 79 women (56%) had live births after IUI (RR 0.68, 95% CI: 0.52-0.88; RD -18%, 95% CI: -30% to -6%).
Limitations, reasons for caution: The study was non-blinded owing to the nature of the interventions. We consider it unlikely that this has introduced performance bias, since pregnancy outcomes are objective outcome measures.
Wider implications of the findings: Since ICI in the natural cycle was inferior to IUI in the natural cycle with cryopreserved donor sperm in terms of live birth rate, IUI is the preferred treatment.
Study funding/competing interest(s): This trial received funding from the Dutch Organization for Health Research and Development (ZonMw project number 837002407). B.W.J.M. is supported by an NHMRC Investigator grant (GNT1176437), reports consultancy for ObsEva and has received research funding from Guerbet, Ferring and Merck. The other authors do not declare a COI.
Trial registration number: NTR4462.
Trial registration date: 11 March 2014.
Date of first patient’s enrolment: 03 June 2014.
Keywords: IUI; cryopreserved donor sperm; donor sperm; donor sperm treatment; intracervical insemination; intrauterine insemination; live birth rate; natural cycle.
© The Author(s) 2022. Published by Oxford University Press on behalf of European Society of Human Reproduction and Embryology. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
References
-
- ASRM. Practice Committee of American Society for Reproductive, Medicine Practice Committee of Society for Assisted Reproductive, Technology Recommendations for gamete and embryo donation: a committee opinion. Fertil Steril 2013;99:47–62. - PubMed
-
- De Geyter C, Calhaz-Jorge C, Kupka MS, Wyns C, Mocanu E, Motrenko T, Scaravelli G, Smeenk J, Vidakovic S, Goossens V; The European IVF-monitoring Consortium (EIM) for the European Society of Human Reproduction and Embryology (ESHRE). ART in Europe, 2015: results generated from European registries by ESHRE. Hum Reprod Open 2020;2020:hoz038. - PMC - PubMed
-
- EU (2004/23/EC). EU Tisue DIRECTIVE 2004/23/EC OF THE EUROPEAN PARLIAMENT AND OF THE COUNCIL on setting standards of quality and safety for the donation, procurement, testing, processing, preservation, storage and distribution of human tissues and cells.
-
- EuropeanUnion. EU Tissue and cell directive, Human Tissue (Quality and Safety for human application) regulations. 2004.
-
- Hurd WW, Randolph JF Jr, Ansbacher R, Menge AC, Ohl DA, Brown AN.. Comparison of intracervical, intrauterine, and intratubal techniques for donor insemination. Fertil Steril 1993;59:339–342. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
