

Clinical re-biopsy of segmental gains-the primary source of preimplantation genetic testing false positives
- PMID: 35460491
- PMCID: PMC9174409
- DOI: 10.1007/s10815-022-02487-z
Clinical re-biopsy of segmental gains-the primary source of preimplantation genetic testing false positives
Abstract
Purpose: Does re-biopsy of blastocysts classified as abnormal (ABN) due to segmental aneuploidy (SA) have clinical utility?
Methods: The live birth (LB) outcomes of mosaic SAs, compared to other categories, were determined after transfer of 3084 PGT-A tested blastocysts. An initial 12-month trial thawed 111 blastocysts classified as ABN due to a SA for clinical re-biopsy, with an additional 58 from a subsequent 16-month revised protocol. Where re-biopsy failed to corroborate the original classification, blastocysts were reported as mosaic and suitable for clinical use.
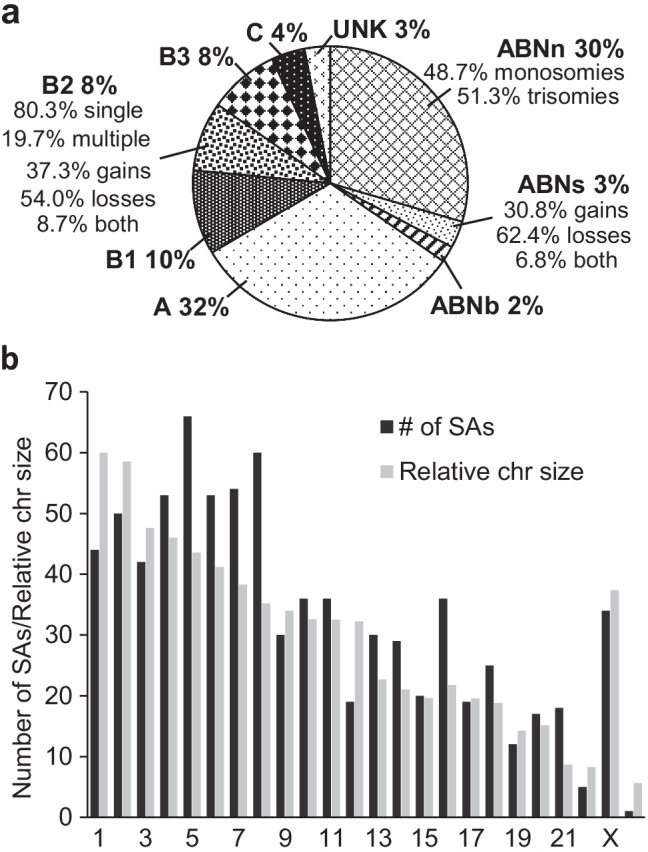
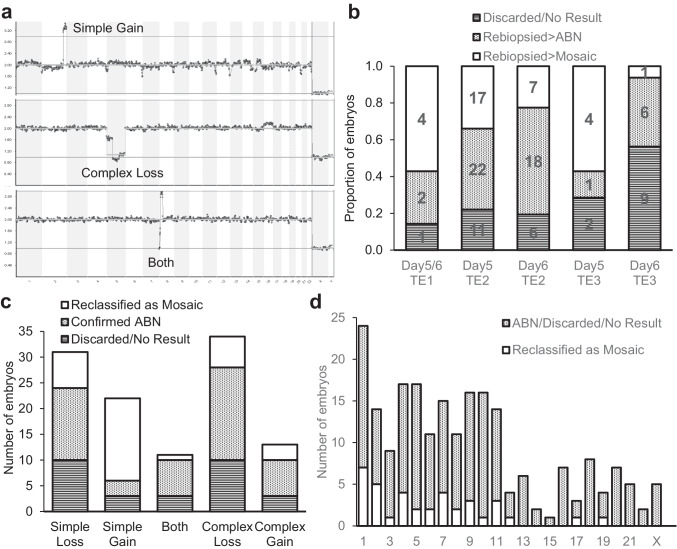
Results: Segmental mosaics had a LB rate (54.1%) which was indistinguishable from that of euploid (53.7%). Numeric mosaics had statistically significant (P < 0.05) reduced LB rates compared to euploid, with high-level numerics (19.2%) also exhibiting a significant reduction compared to low level (42.3%). Of the initial 111 blastocysts with SAs, 85 could be re-biopsied. Segmental gains became suitable for re-biopsy at a high rate (90.9%), with 84.2% (16/19) of these reclassified as mosaic. Only 73.0% of deletions and complex changes were suitable for re-biopsy, of which 73.0% (46/63) were confirmed ABN. The subsequent 16-month period primarily focused on gains, confirming the high rate at which they can be reclassified as clinically useable.
Conclusions: Blastocysts harboring mosaic segmental duplications, rather than SAs in general, are the primary source of false-positive PGT-A results and represent a category with a LB rate similar to that of euploid. A high degree of confidence in the reliability of PGT-A results can be maintained by performing confirmatory clinical TE biopsies.
Keywords: Clinical re-biopsy; False positives; Mosaicism; Preimplantation genetic testing; Segmental aneuploidy.
© 2022. The Author(s), under exclusive licence to Springer Science+Business Media, LLC, part of Springer Nature.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Srebniak MI, Joosten M, Knapen MFCM, Arends LR, Polak M, van Veen S, et al. Frequency of submicroscopic chromosomal aberrations in pregnancies without increased risk for structural chromosomal aberrations: systematic review and meta-analysis. Ultrasound Obstet Gynecol. 2018;51:445–452. doi: 10.1002/uog.17533. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
