

Molecular biomarker-defined brain tumors: Epidemiology, validity, and completeness in the United States
- PMID: 35460555
- PMCID: PMC9629432
- DOI: 10.1093/neuonc/noac113
Molecular biomarker-defined brain tumors: Epidemiology, validity, and completeness in the United States
Erratum in
-
Corrigendum to: Molecular biomarker-defined brain tumors: Epidemiology, validity, and completeness in the United States.Neuro Oncol. 2023 Feb 14;25(2):424-429. doi: 10.1093/neuonc/noac270. Neuro Oncol. 2023. PMID: 36534983 Free PMC article. No abstract available.
Abstract
Background: Selected molecular biomarkers were incorporated into the US cancer registry reporting for patients with brain tumors beginning in 2018. We investigated the completeness and validity of these variables and described the epidemiology of molecularly defined brain tumor types.
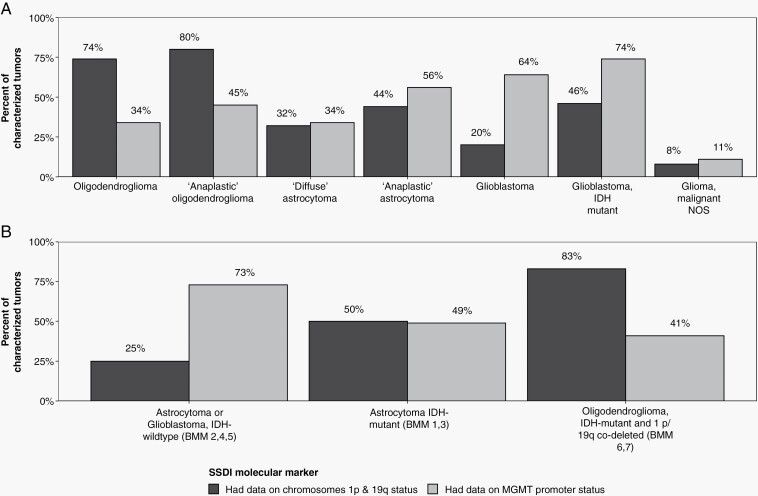
Methods: Brain tumor patients with histopathologically confirmed diagnosis in 2018 were identified within the Central Brain Tumor Registry of the United States and NCI's Surveillance, Epidemiology, and End Results Incidence databases. The brain molecular markers (BMM) site-specific data item was assessed for coding completeness and validity. 1p/19q status, MGMT promoter methylation, WHO grade data items, and new ICD-O-3 codes were additionally evaluated. These data were used to profile the characteristics and age-adjusted incidence rates per 100 000 population of molecularly defined brain tumors with 95% confidence intervals (95% CI).
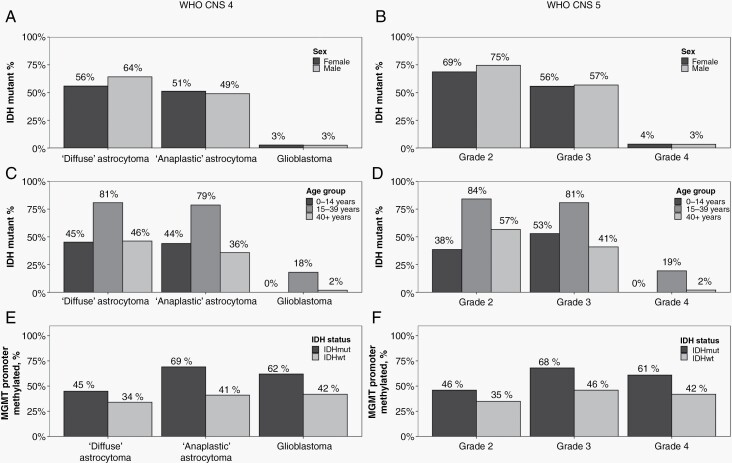
Results: BMM completeness across the applicable tumor types was 75%-92% and demonstrated favorable coding validity. IDH-wildtype glioblastomas' incidence rate was 1.74 (95% CI: 1.69-1.78), as compared to 0.14 for WHO grade 2 (95% CI: 0.12-0.15), 0.15 for grade 3 (95% CI: 0.14-0.16), and 0.07 for grade 4 (95% CI: 0.06-0.08) IDH-mutant astrocytomas. Irrespective of WHO grade, IDH mutation prevalence was highest in adolescent and young adult patients, and IDH-mutant astrocytomas were more frequently MGMT promoter methylated. Among pediatric-type tumors, the incidence rate was 0.06 for H3K27M-mutant diffuse midline gliomas (95% CI: 0.05-0.07), 0.03 for SHH-activated/TP53-wildtype medulloblastomas (95% CI: 0.02-0.03), and <0.01 for both C19MC-altered embryonal tumor with multilayered rosettes and RELA-fusion ependymomas.
Conclusions: Our findings illustrate the success of developing a dedicated, integrated diagnosis variable, which provides critical molecular information about brain tumors related to accurate diagnosis.
Keywords: CBTRUS; IDH; biomarkers; brain tumor; molecular epidemiology.
Published by Oxford University Press on behalf of the Society for Neuro-Oncology 2022.
Figures
References
-
- Jenkins RB, Blair H, Ballman KV, et al. A t(1;19)(q10;p10) mediates the combined deletions of 1p and 19q and predicts a better prognosis of patients with oligodendroglioma. Cancer Res. 2006;66(20):9852–9861. - PubMed
-
- van den Bent MJ, Brandes AA, Taphoorn MJ, et al. Adjuvant procarbazine, lomustine, and vincristine chemotherapy in newly diagnosed anaplastic oligodendroglioma: long-term follow-up of EORTC brain tumor group study 26951. J Clin Oncol. 2013;31(3):344–350. - PubMed
-
- Hartmann C, Hentschel B, Wick W, et al. Patients with IDH1 wild type anaplastic astrocytomas exhibit worse prognosis than IDH1-mutated glioblastomas, and IDH1 mutation status accounts for the unfavorable prognostic effect of higher age: implications for classification of gliomas. Acta Neuropathol. 2010;120(6):707–718. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
