

Semi-prone thoracoscopic esophagectomy for esophageal carcinoma with aberrant right subclavian artery and non-recurrent inferior laryngeal nerve
- PMID: 35461251
- PMCID: PMC9034527
- DOI: 10.1186/s13019-022-01829-3
Semi-prone thoracoscopic esophagectomy for esophageal carcinoma with aberrant right subclavian artery and non-recurrent inferior laryngeal nerve
Abstract
Background: Aberrant right subclavian artery (ARSA) accompanied by non-recurrent inferior laryngeal nerve (NRILN) is a rare anomaly. In cases of thoracic esophageal carcinoma associated with ARSA and NRILN, surgeons must take extra care not to injury these vessels and nerves. We believe semi-prone thoracoscopic esophagectomy to be a surgical approach that can safely deal with such an anomaly.
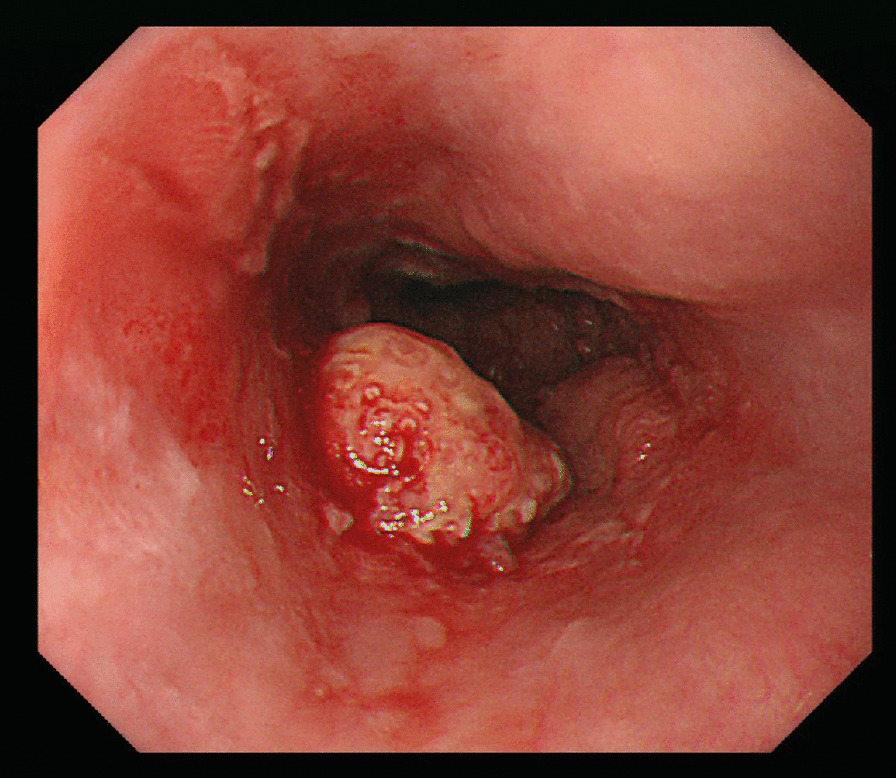
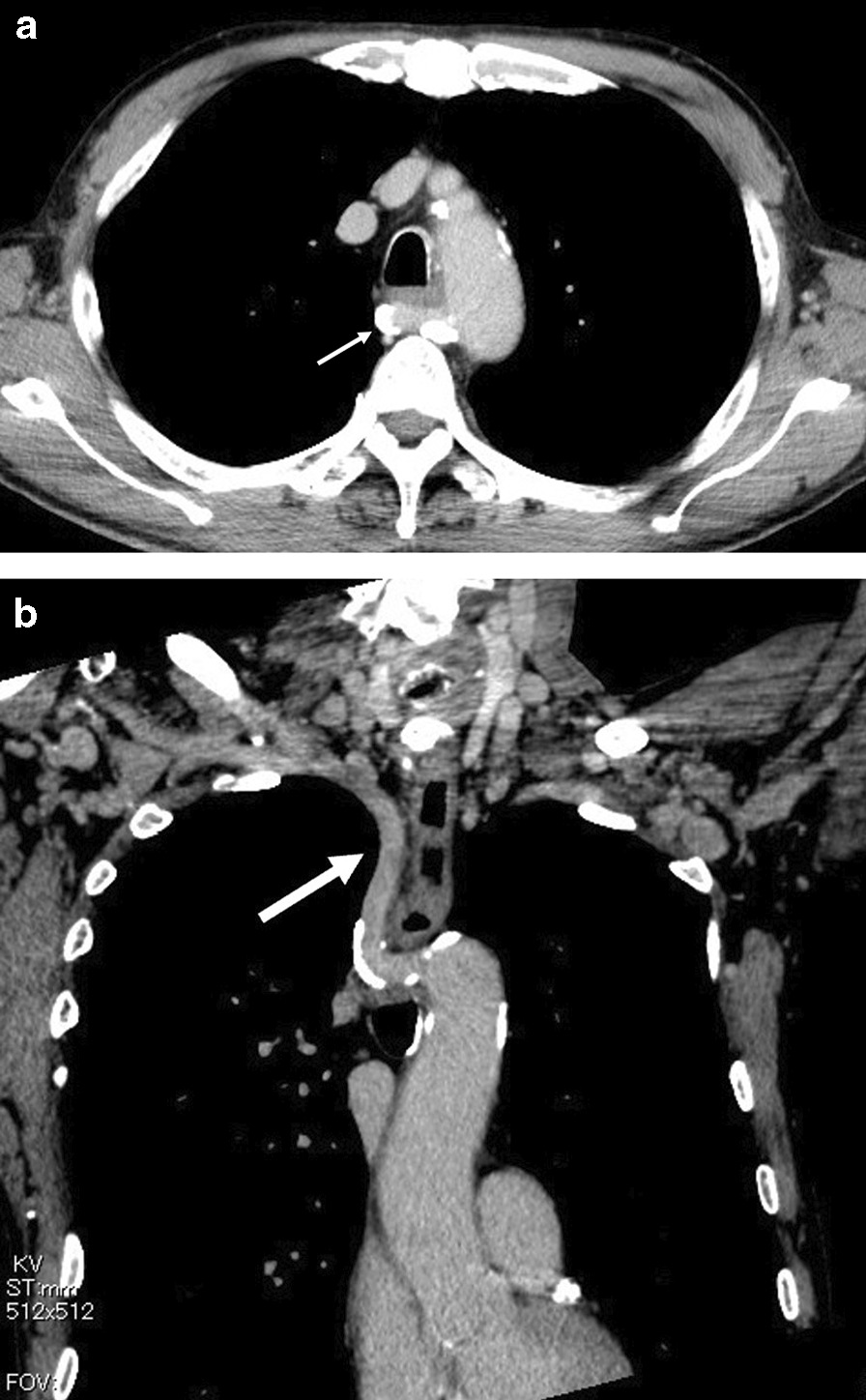
Case presentation: A 70-year-old man complained of feelings of chest constriction. Endoscopic examination revealed an esophageal tumor and computed tomography showed an ARSA. We performed semi-prone thoracoscopic esophagectomy for case with ARSA and NRILN. We identified these anomalies during esophagectomy, and we could complete surgery without injury these vessels and nerves. The patient had an uneventful recovery and discharged 22 days after surgery.
Conclusions: Semi-prone thoracoscopic esophagectomy for esophageal carcinoma can be performed safely with a wide operative field, and is an excellent procedure for dissecting esophageal carcinoma in patients with ARSA and NRILN.
Keywords: Aberrant right subclavian artery; Esophageal carcinoma; Non-recurrent inferior laryngeal nerve; Semi-prone; Thoracoscopic esophagectomy.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


Similar articles
-
Cervical-First Approach in Thoracoscopic Esophagectomy With Intraoperative Nerve Monitoring for an Esophageal Cancer Patient With Aberrant Right Subclavian Artery.Asian J Endosc Surg. 2025 Jan-Dec;18(1):e70018. doi: 10.1111/ases.70018. Asian J Endosc Surg. 2025. PMID: 39757543
-
Safe Resection of Esophageal Cancer with a Non-Recurrent Inferior Laryngeal Nerve Associated with an Aberrant Right Subclavian Artery Using Intraoperative Nerve Monitoring.Acta Med Okayama. 2025 Apr;79(2):139-144. doi: 10.18926/AMO/68654. Acta Med Okayama. 2025. PMID: 40302287
-
Neck Dissection and Thoracoscopic Esophagectomy in Esophageal Cancer with Aberrant Subclavian Artery.Anticancer Res. 2017 Jul;37(7):3787-3790. doi: 10.21873/anticanres.11754. Anticancer Res. 2017. PMID: 28668875
-
Preoperative diagnosis of right nonrecurrent inferior laryngeal nerve by CT scan: report of a case and review of the literature.J Med Liban. 2007 Jan-Mar;55(1):46-9. J Med Liban. 2007. PMID: 17489307 Review.
-
Anatomical variation in the right non-recurrent laryngeal nerve reported from studies using pre-operative arterial imaging.Surg Radiol Anat. 2019 Aug;41(8):943-949. doi: 10.1007/s00276-019-02252-5. Epub 2019 May 13. Surg Radiol Anat. 2019. PMID: 31087139
References
-
- Tamachi T, Hoshino I, Kono T, et al. A case of esophageal carcinoma with aberrant right subclavian artery. J Jpn Surg Assoc. 2013;74:2755–2760. doi: 10.3919/jjsa.74.2755. - DOI
-
- Mizuuchi Y, Watanabe M, Suehara N, et al. A case of prone thoracoscopic esophagectomy for esophageal carcinoma with aberrant right subclavian artery and nonrecurrent inferior laryngeal nerve. J Jpn Surg Assoc. 2010;71:654–658. doi: 10.3919/jjsa.71.654. - DOI
-
- Ujiie N, Kikuchi H, Watanabe T, et al. A case of a right subclavian artery-anastomotic fistula associated with the aberrant subclavian artery developed after radical operation for esophageal cancer. J Jpn Surg Assoc. 2014;75:1836–1839. doi: 10.3919/jjsa.75.1836. - DOI
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
