

Individualized prediction of psychiatric readmissions for patients with major depressive disorder: a 10-year retrospective cohort study
- PMID: 35461305
- PMCID: PMC9035153
- DOI: 10.1038/s41398-022-01937-7
Individualized prediction of psychiatric readmissions for patients with major depressive disorder: a 10-year retrospective cohort study
Abstract
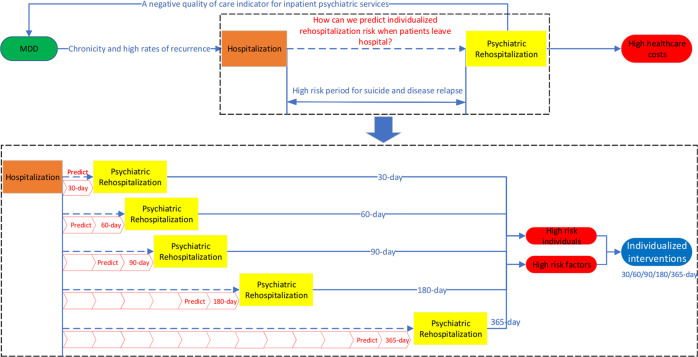
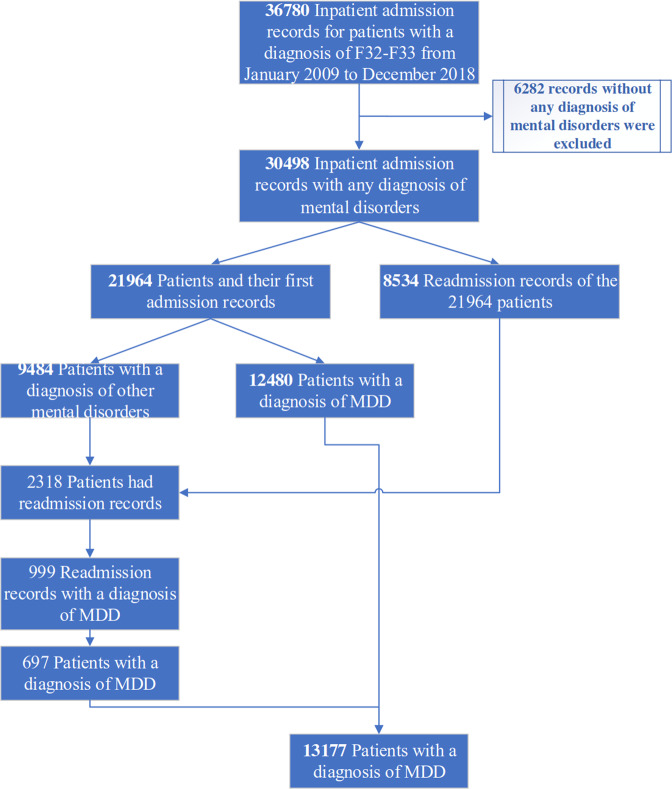
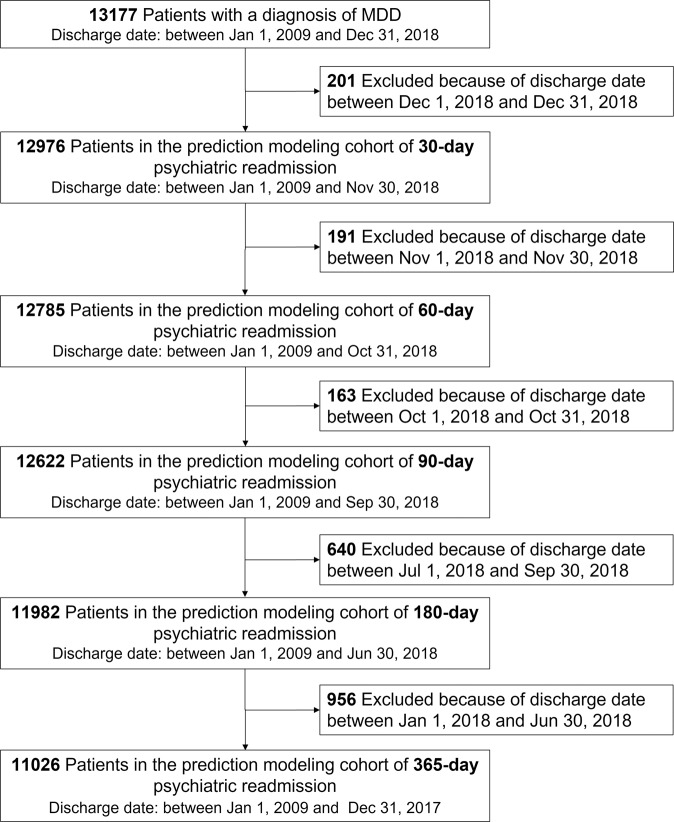
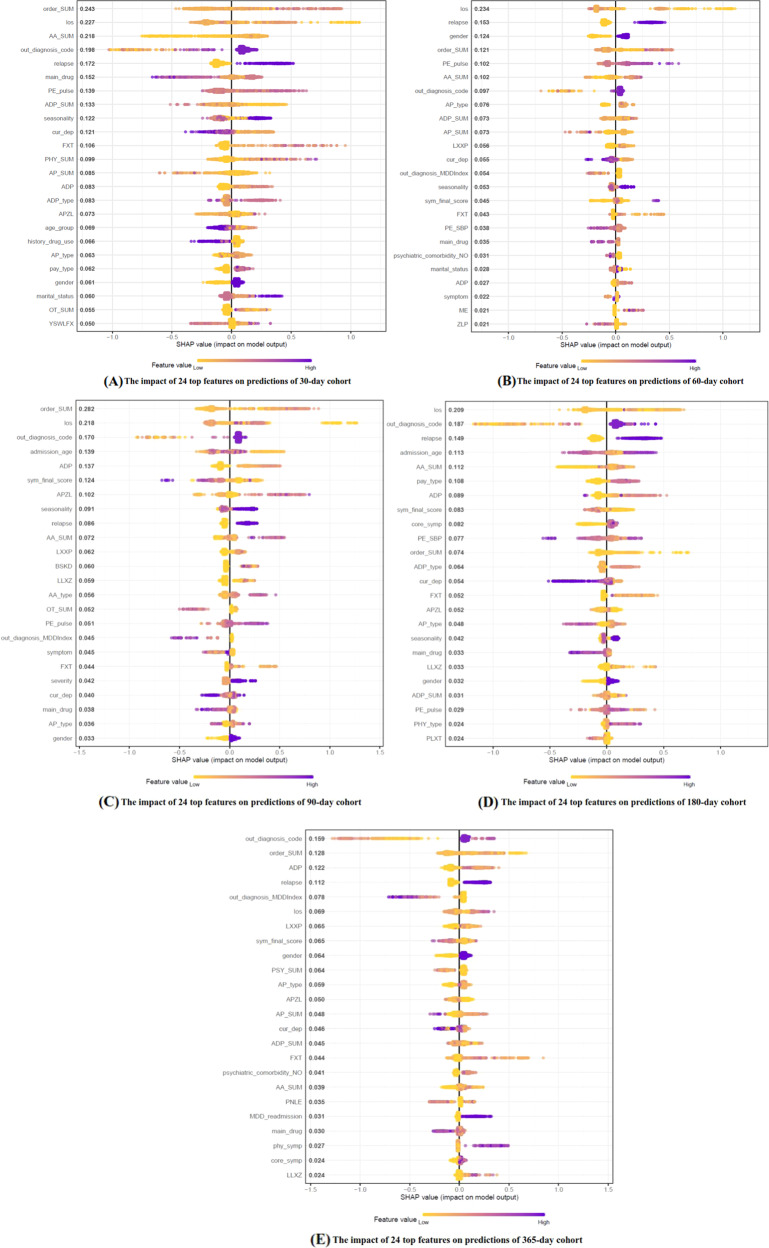
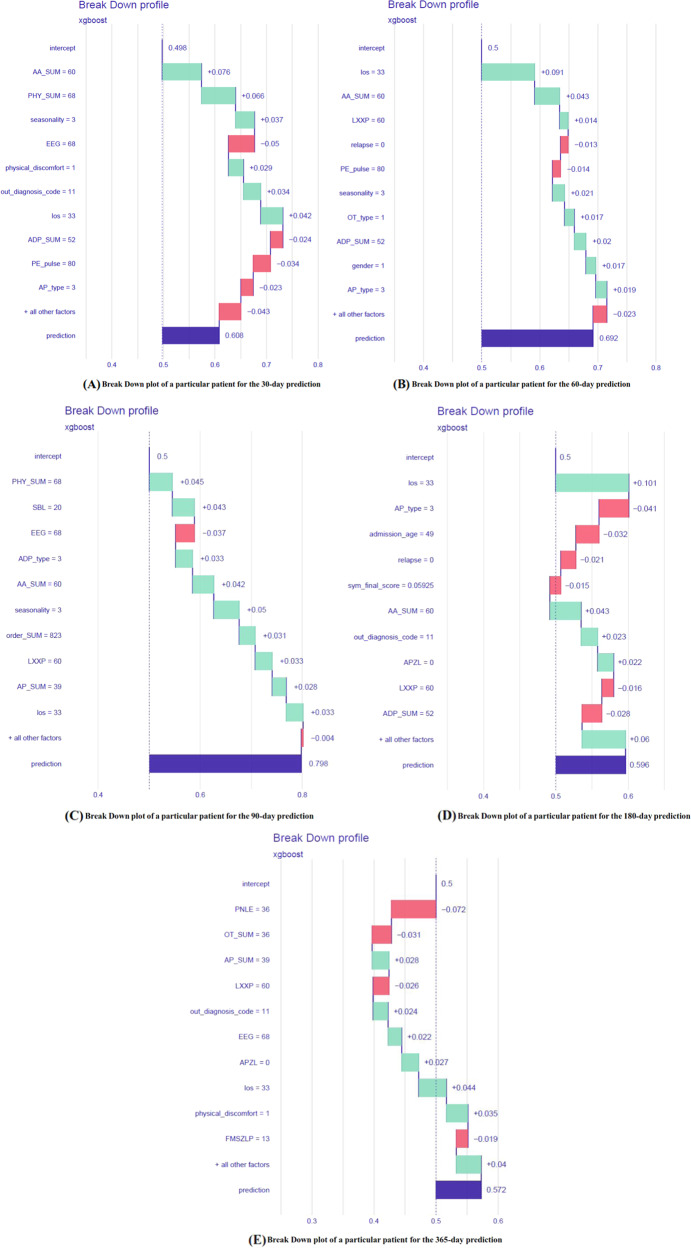
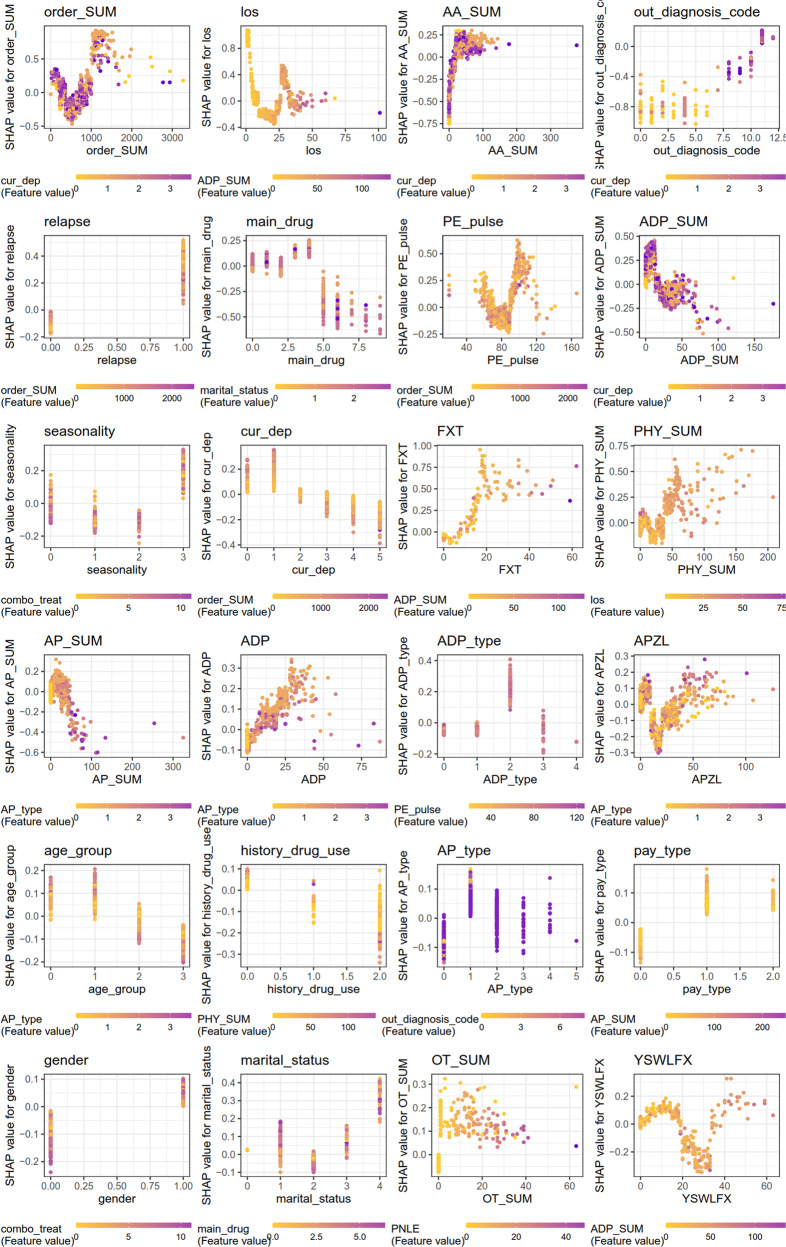
Patients with major depressive disorder (MDD) are at high risk of psychiatric readmission while the factors associated with such adverse illness trajectories and the impact of the same factor at different follow-up times remain unclear. Based on machine learning (ML) approaches and real-world electronic medical records (EMR), we aimed to predict individual psychiatric readmission within 30, 60, 90, 180, and 365 days of an initial major depression hospitalization. In addition, we examined to what extent our prediction model could be made interpretable by quantifying and visualizing the features that drive the predictions at different follow-up times. By identifying 13,177 individuals discharged from a hospital located in western China between 2009 and 2018 with a recorded diagnosis of MDD, we established five prediction-modeling cohorts with different follow-up times. Four different ML models were trained with features extracted from the EMR, and explainable methods (SHAP and Break Down) were utilized to analyze the contribution of each of the features at both population-level and individual-level. The model showed a performance on the holdout testing dataset that decreased over follow-up time after discharge: AUC 0.814 (0.758-0.87) within 30 days, AUC 0.780 (0.728-0.833) within 60 days, AUC 0.798 (0.75-0.846) within 90 days, AUC 0.740 (0.687-0.794) within 180 days, and AUC 0.711 (0.676-0.747) within 365 days. Results add evidence that markers of depression severity and symptoms (recurrence of the symptoms, combination of key symptoms, the number of core symptoms and physical symptoms), along with age, gender, type of payment, length of stay, comorbidity, treatment patterns such as the use of anxiolytics, antipsychotics, antidepressants (especially Fluoxetine, Clonazepam, Olanzapine, and Alprazolam), physiotherapy, and psychotherapy, and vital signs like pulse and SBP, may improve prediction of psychiatric readmission. Some features can drive the prediction towards readmission at one follow-up time and towards non-readmission at another. Using such a model for decision support gives the clinician dynamic information of the patient's risk of psychiatric readmission and the specific features pulling towards readmission. This finding points to the potential of establishing personalized interventions that change with follow-up time.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- H Whiteford, Addressing the burden of mental, neurological, and substance use disorders: Key messages from disease control priorities, 3rd edition, Lancet. 2015. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
