

Validation of the myocardial-ischaemic-injury-index machine learning algorithm to guide the diagnosis of myocardial infarction in a heterogenous population: a prespecified exploratory analysis
- PMID: 35461689
- PMCID: PMC9052331
- DOI: 10.1016/S2589-7500(22)00025-5
Validation of the myocardial-ischaemic-injury-index machine learning algorithm to guide the diagnosis of myocardial infarction in a heterogenous population: a prespecified exploratory analysis
Abstract
Background: Diagnostic pathways for myocardial infarction rely on fixed troponin thresholds, which do not recognise that troponin varies by age, sex, and time within individuals. To overcome this limitation, we recently introduced a machine learning algorithm that predicts the likelihood of myocardial infarction. Our aim was to evaluate whether this algorithm performs well in routine clinical practice and predicts subsequent events.
Methods: The myocardial-ischaemic-injury-index (MI3) algorithm was validated in a prespecified exploratory analysis using data from a multi-centre randomised trial done in Scotland, UK that included consecutive patients with suspected acute coronary syndrome undergoing serial high-sensitivity cardiac troponin I measurement. Patients with ST-segment elevation myocardial infarction were excluded. MI3 incorporates age, sex, and two troponin measurements to compute a value (0-100) reflecting an individual's likelihood of myocardial infarction during the index visit and estimates diagnostic performance metrics (including area under the receiver-operating-characteristic curve, and the sensitivity, specificity, negative predictive value, and positive predictive value) at the computed score. Model performance for an index diagnosis of myocardial infarction (type 1 or type 4b), and for subsequent myocardial infarction or cardiovascular death at 1 year was determined using the previously defined low-probability threshold (1·6) and high-probability MI3 threshold (49·7). The trial is registered with ClinicalTrials.gov, NCT01852123.
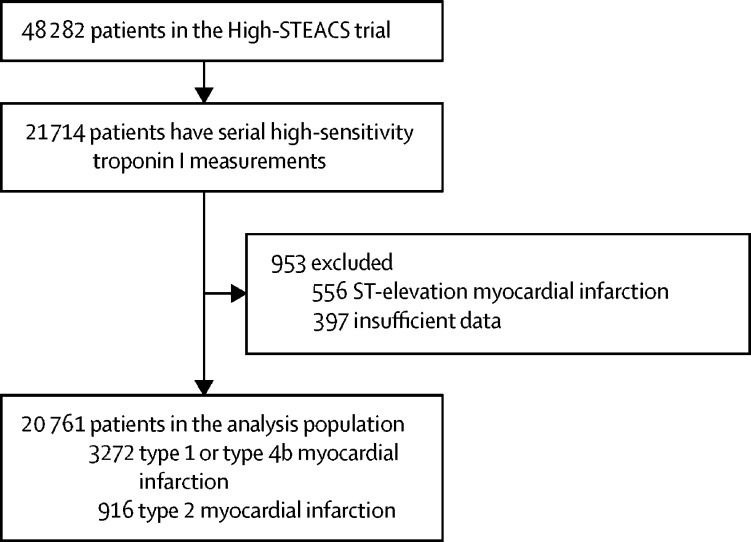
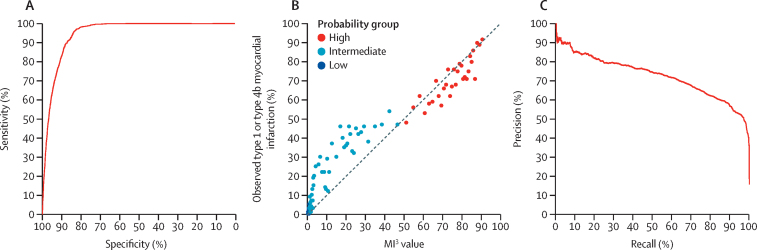
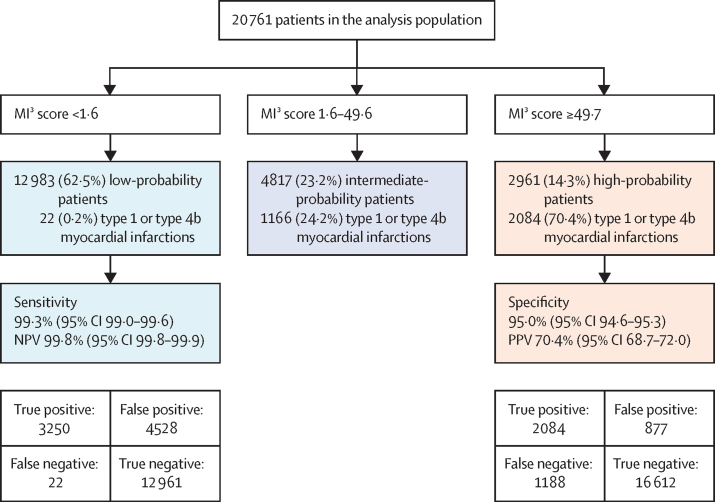
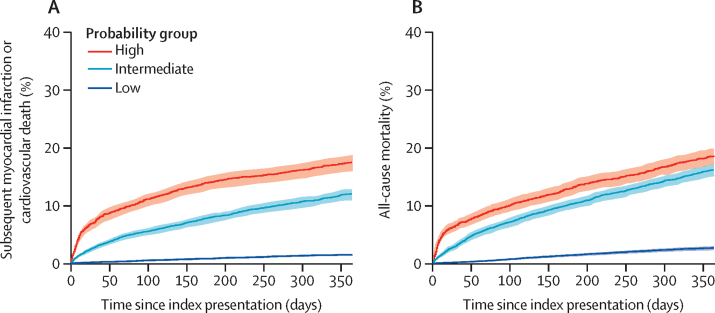
Findings: In total, 20 761 patients (64 years [SD 16], 9597 [46%] women) enrolled between June 10, 2013, and March 3, 2016, were included from the High-STEACS trial cohort, of whom 3272 (15·8%) had myocardial infarction. MI3 had an area under the receiver-operating-characteristic curve of 0·949 (95% CI 0·946-0·952) identifying 12 983 (62·5%) patients as low-probability for myocardial infarction at the pre-specified threshold (MI3 score <1·6; sensitivity 99·3% [95% CI 99·0-99·6], negative predictive value 99·8% [99·8-99·9]), and 2961 (14·3%) as high-probability at the pre-specified threshold (MI3 score ≥49·7; specificity 95·0% [94·6-95·3], positive predictive value 70·4% [68·7-72·0]). At 1 year, subsequent myocardial infarction or cardiovascular death occurred more often in high-probability patients than low-probability patients (520 [17·6%] of 2961 vs 197 [1·5%] of 12 983], p<0·0001).
Interpretation: In consecutive patients undergoing serial cardiac troponin measurement for suspected acute coronary syndrome, the MI3 algorithm accurately estimated the likelihood of myocardial infarction and predicted subsequent adverse cardiovascular events. By providing individual probabilities the MI3 algorithm could improve the diagnosis and assessment of risk in patients with suspected acute coronary syndrome.
Funding: Medical Research Council, British Heart Foundation, National Institute for Health Research, and NHSX.
Copyright © 2022 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests NLM has received honoraria or consultancy from Abbott Diagnostics, Roche Diagnostics, Siemens Healthineers, and LumiraDx. KKL has received honoraria from Abbott Diagnostics. ASVS's institution (the University of Edinburgh) has received speaker fees from Abbott Diagnostics. JWP has undertaken consultancy for Abbott Diagnostics. MPT has received consulting fees, honoraria, or payment from Abbott, Roche, and Siemens; funding for clinical research from Radiometer; and participated on a data safety monitoring board or an advisory board for Abbott, Radiometer, Roche, and Siemens. All other authors declare no competing interests.
Figures
Comment in
-
Moving forward with machine learning models in acute chest pain.Lancet Digit Health. 2022 May;4(5):e291-e292. doi: 10.1016/S2589-7500(22)00046-2. Lancet Digit Health. 2022. PMID: 35461685 No abstract available.
References
-
- Collet JP, Thiele H, Barbato E, et al. The ‘Ten Commandments’ for the 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J. 2020;41:3495–3497. - PubMed
-
- Body R, Carley S, McDowell G, et al. Rapid exclusion of acute myocardial infarction in patients with undetectable troponin using a high-sensitivity assay. J Am Coll Cardiol. 2011;58:1332–1339. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
