

Characteristics and outcomes of ambulatory patients with suspected COVID-19 at a respiratory referral center
- PMID: 35462298
- PMCID: PMC8986541
- DOI: 10.1016/j.rmed.2022.106832
Characteristics and outcomes of ambulatory patients with suspected COVID-19 at a respiratory referral center
Abstract
Rationale: SARS-CoV-2 continues to cause a global pandemic and management of COVID-19 in outpatient settings remains challenging.
Objective: We sought to describe characteristics of patients with chronic respiratory disease (CRD) experiencing symptoms consistent with COVID-19, who were seen in a novel Acute Respiratory Clinic, prior to widely available testing, emergence of variants, COVID-19 vaccination, and post-vaccination (breakthrough) SARS-CoV-2 infections.
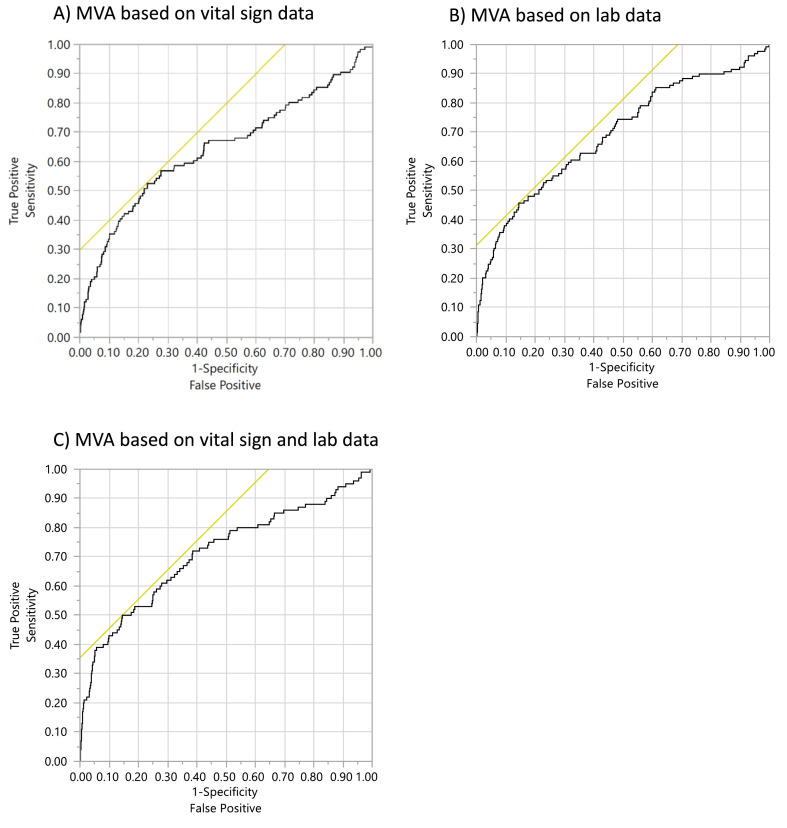
Methods: Retrospective electronic medical record data were analyzed from 907 adults with presumed COVID-19 seen between March 16, 2020 and January 7, 2021. Data included demographics, comorbidities, medications, vital signs, laboratory tests, pulmonary function tests, patient disposition, and co-infections. The overdispersed data (aod) R package was used to create a logit model using COVID-19 diagnosis by PCR as the dichotomous outcome variable. Univariate, conventional multivariate and elastic net machine learning were used to analyze data.
Results: Male gender, elevated baseline temperature, and respiratory rate predicted COVID-19 diagnosis. Eosinopenia, neutrophilia, and lymphocytosis were also associated with COVID-19 diagnosis. However, asthma and COPD diagnoses were not associated with SARS-CoV-2 PCR positive test. Male gender, low oxygen saturation, and lower forced expiratory volume in 1 s (FEV1) were associated with higher hospital referral.
Conclusions: CRD patients with acute respiratory symptoms in the ambulatory setting were more likely to have COVID-19 if male, febrile and tachypneic. Patients with lower pre-morbid FEV1 and lower SPO2 are more likely to be referred to the hospital. A composite of vitals sigs and WBC differential help risk stratify CRD patients seeking care for presumed COVID-19.
Keywords: Ambulatory respiratory infections; COVID-19; Clinical prediction.
Copyright © 2022 Elsevier Ltd. All rights reserved.
Conflict of interest statement
No conflicts with this manuscript.
Figures


References
-
- WHO Coronavirus disease (COVID-19) pandemic. https://www.who.int/emergencies/diseases/novel-coronavirus-2019 [Available from:
-
- Bentivegna M., Hulme C., Ebell M.H. Primary care relevant risk factors for adverse outcomes in patients with COVID-19 infection: a systematic review. J. Am. Board Fam. Med. 2021;34(Suppl):S113–S126. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
