

The Effect of Borderline Pulmonary Hypertension on Survival in Chronic Lung Disease
- PMID: 35462365
- PMCID: PMC9533441
- DOI: 10.1159/000524263
The Effect of Borderline Pulmonary Hypertension on Survival in Chronic Lung Disease
Abstract
Background: The impact of the new "borderline" hemodynamic class for pulmonary hypertension (PH) (mean pulmonary artery pressure [mPAP], 21-24 mm Hg and pulmonary vascular resistance, [PVR], ≥3 wood units, [WU]) in chronic obstructive pulmonary disease (COPD) and interstitial lung disease (ILD) is unclear.
Objectives: The aim of this study was to assess the effect of borderline PH (BLPH) on survival in COPD and ILD patients.
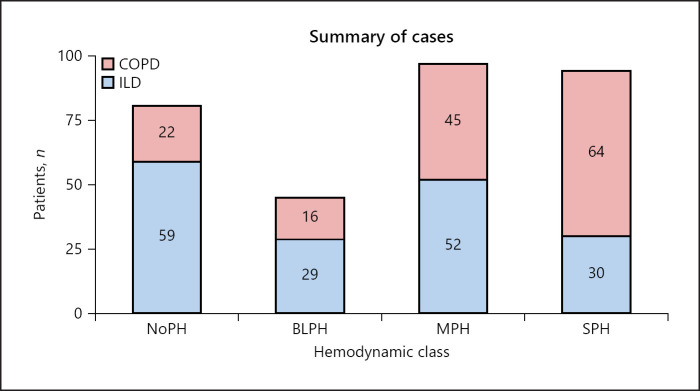
Method: Survival was analyzed from retrospective data from 317 patients in 12 centers (Italy, Spain, UK) comparing four hemodynamic groups: the absence of PH (NoPH; mPAP <21 mm Hg or 21-24 mm Hg and PVR <3 WU), BLPH (mPAP 21-24 mm Hg and PVR ≥3 WU), mild-moderate PH (MPH; mPAP 25-35 mm Hg and cardiac index [CI] ≥2 L/min/m2), and severe PH (SPH; mPAP ≥35 mm Hg or mPAP ≥25 mm Hg and CI <2 L/min/m2).
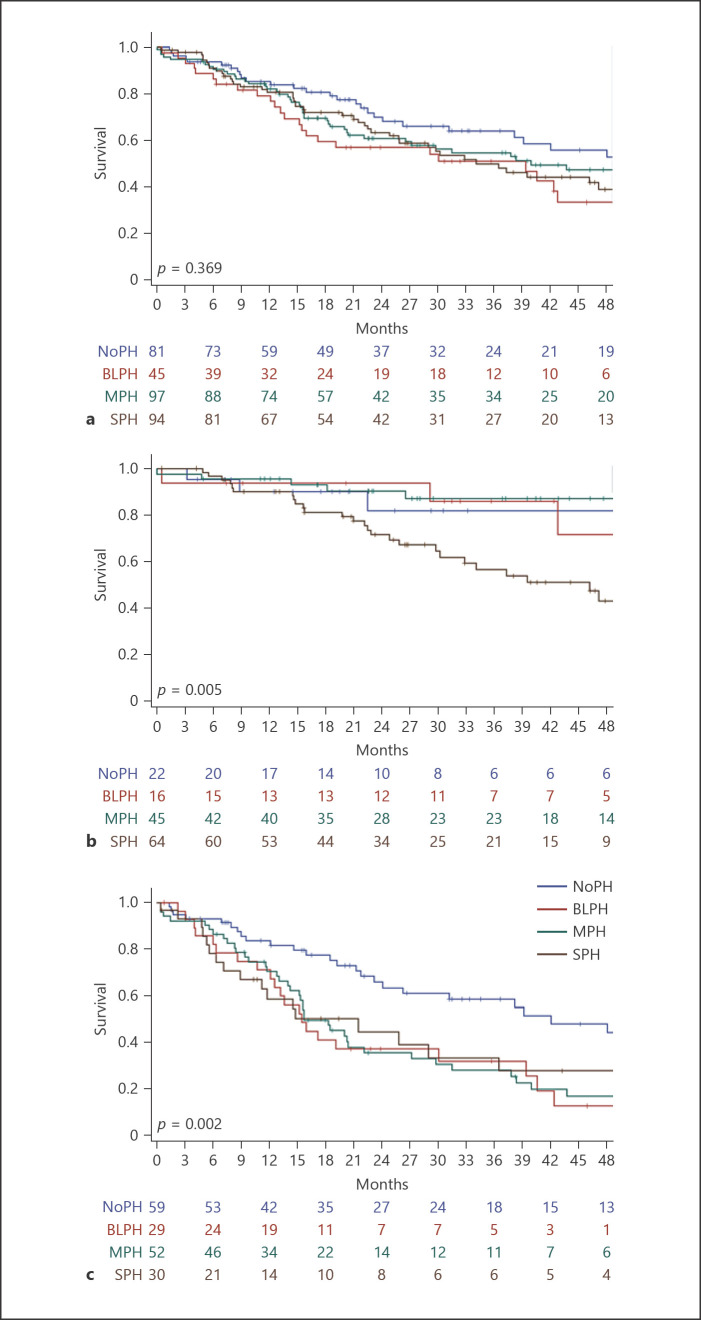
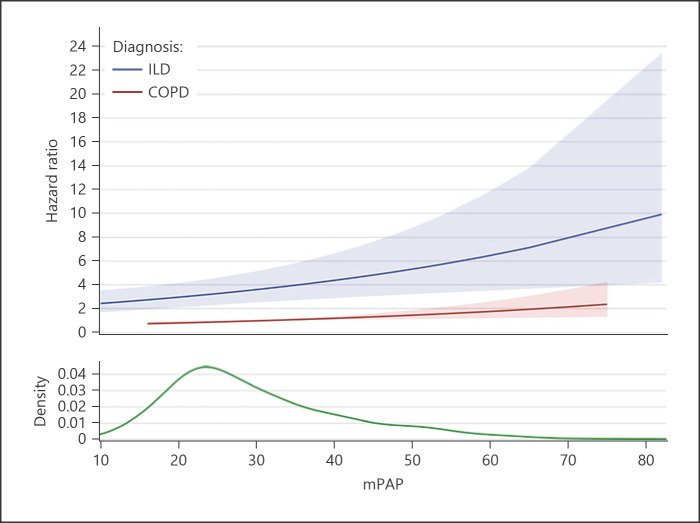
Results: BLPH affected 14% of patients; hemodynamic severity did not predict survival when COPD and ILD patients were analyzed together. However, survival in the ILD cohort for any PH level was worse than in NoPH (3-year survival: NoPH 58%, BLPH 32%, MPH 28%, SPH 33%, p = 0.002). In the COPD cohort, only SPH had reduced survival compared to the other groups (3-year survival: NoPH 82%, BLPH 86%, MPH 87%, SPH 57%, p = 0.005). The mortality risk correlated significantly with mPAP in ILD (hazard ratio [HR]: 2.776, 95% CI: 2.057-3.748, p < 0.001) and notably less in COPD patients (HR: 1.015, 95% CI: 1.003-1.027, p = 0.0146).
Conclusions: In ILD, any level of PH portends worse survival, while in COPD, only SPH presents a worse outcome.
Keywords: Borderline pulmonary hypertension; Chronic lung disease; Chronic obstructive pulmonary disease; Interstitial lung disease; Survival.
© 2022 The Author(s). Published by S. Karger AG, Basel.
Conflict of interest statement
Dr. Piccari reports grants, personal fees, and nonfinancial support from Janssen and nonfinancial support from Menarini, outside the submitted work. Dr. Wort reports grants and personal fees from Actelion UK. He has also received personal fees from MSD, Janssen, and GSK, outside the submitted work. Dr. Price reports personal fees from Janssen, outside the submitted work. Dr. Meloni, Dr. Rizzo, Dr. Martino, Dr. Salvaterra, Dr. Scelsi, Dr. López-Meseguer, Dr. Blanco, Dr. Callari, Dr. Pérez González, Dr. Tuzzolino, Dr. McCabe, Dr. Rodríguez-Chiaradía, and Dr. Vitulo, have nothing to disclose.
Figures
References
-
- Kessler R, Faller M, Fourgaut G, Mennecier B, Weitzenblum E. Predictive factors of hospitalization for acute exacerbation in a series of 64 patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1999 Jan;159((1)):158–64. - PubMed
-
- Oswald-Mammosser M, Weitzenblum E, Quoix E, Moser G, Chaouat A, Charpentier C, et al. Prognostic factors in COPD patients receiving long-term oxygen therapy. Importance of pulmonary artery pressure. Chest. 1995 May;107((5)):1193–8. - PubMed
-
- Hurdman J, Condliffe R, Elliot CA, Davies C, Hill C, Wild JM, et al. ASPIRE registry: assessing the spectrum of pulmonary hypertension identified at a REferral centre. Eur Respir J. 2012 Apr;39((4)):945–55. - PubMed
-
- Gall H, Felix JF, Schneck FK, Milger K, Sommer N, Voswinckel R, et al. The giessen pulmonary hypertension registry: survival in pulmonary hypertension subgroups. J Heart Lung Transplant. 2017 Sep;36((9)):957–67. - PubMed
-
- Blanco I, Piccari L, Barberà JA. Pulmonary vasculature in COPD: the silent component. Respirology. 2016 Aug;21((6)):984–94. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
