

High threshold efficacy responses in moderate-to-severe atopic dermatitis are associated with additional quality of life benefits: pooled analyses of abrocitinib monotherapy studies in adults and adolescents
- PMID: 35462428
- PMCID: PMC9539871
- DOI: 10.1111/jdv.18170
High threshold efficacy responses in moderate-to-severe atopic dermatitis are associated with additional quality of life benefits: pooled analyses of abrocitinib monotherapy studies in adults and adolescents
Abstract
Background: Once-daily abrocitinib treatment provided meaningful improvements in signs and symptoms of moderate-to-severe atopic dermatitis (AD) in randomized controlled studies.
Objective: To evaluate proportions of patients with responses meeting higher threshold efficacy responses than commonly used efficacy end points and to determine if these responses were associated with quality-of-life (QoL) benefits.
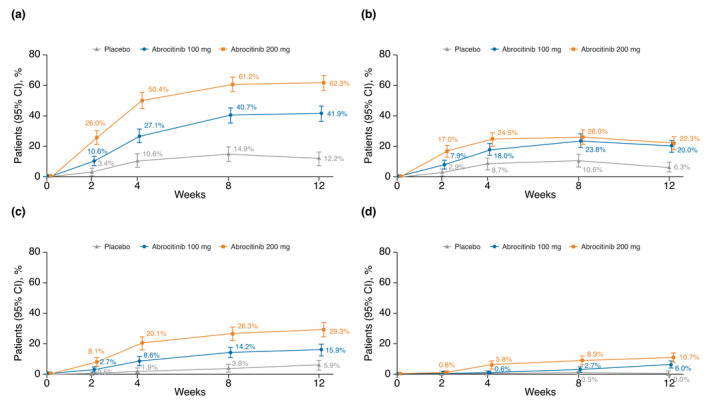
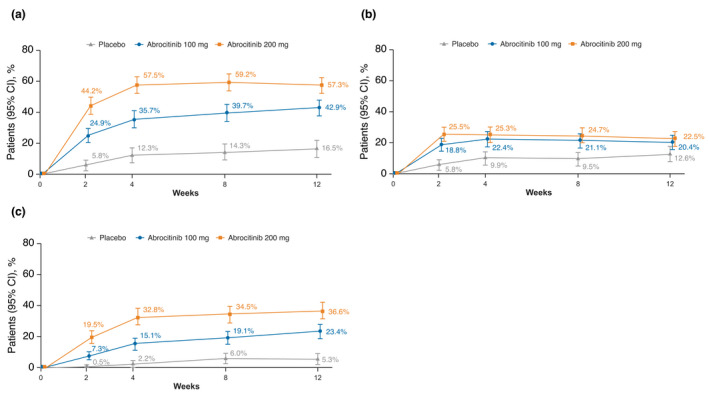
Methods: Data from a phase 2b (NCT02780167) and two phase 3 studies (NCT03349060/JADE MONO-1; NCT03575871/JADE MONO-2) in adult and adolescent patients (N = 942) with moderate-to-severe AD receiving once-daily abrocitinib 200 mg, abrocitinib 100 mg or placebo were pooled. Commonly used (Eczema Area and Severity Index [EASI]-75 and ≥4-point improvement in Pruritus Numerical Rating Scale [PP-NRS4]) and higher threshold efficacy end points (EASI-90 to <EASI-100, EASI-100 or PP-NRS0/1 response) were evaluated. Proportions of patients across Children's Dermatology Life Quality Index/Dermatology Life Quality Index (CDLQI/DLQI) band descriptors who achieved various efficacy end points were analysed.
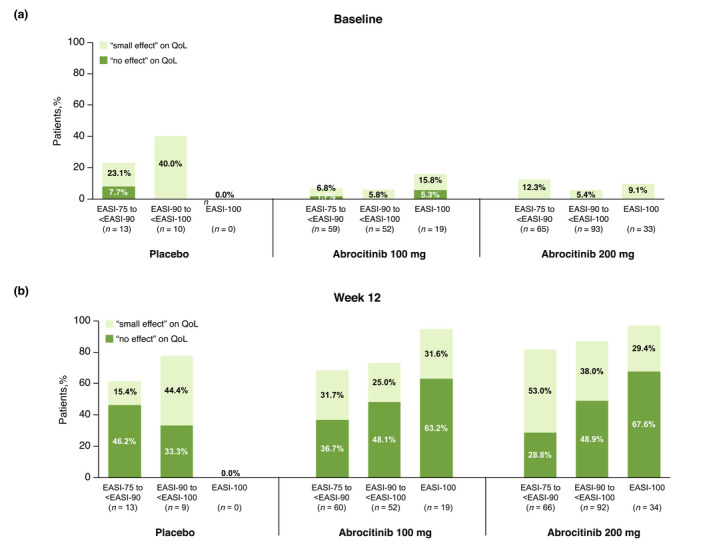
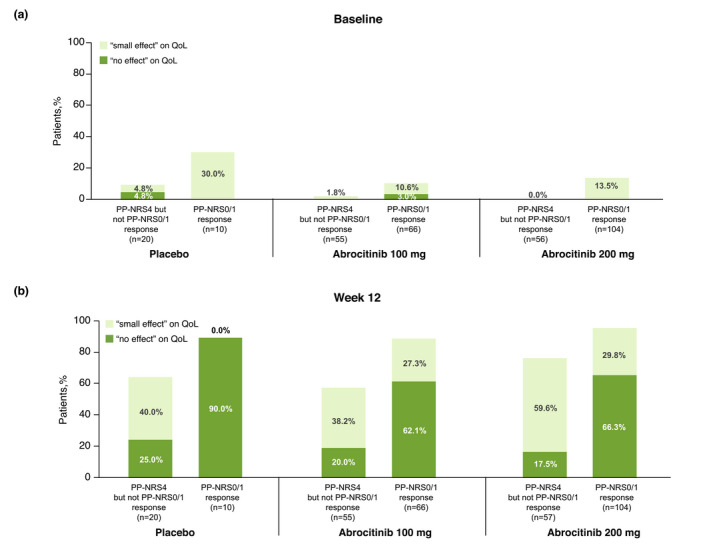
Results: More abrocitinib-treated patients achieved commonly used or higher threshold efficacy end points at week 12 vs. placebo. More abrocitinib-treated patients who achieved higher threshold efficacy end points reported 'no effect' of AD on QoL (by CDLQI/DLQI) at week 12 vs. those who achieved commonly used but not higher threshold efficacy end points (PP-NRS0/1 vs. PP-NRS4 but not PP-NRS0/1 responders [200 mg: 66.3% vs. 17.5%; 100 mg: 62.1% vs. 20.0%]; EASI-100, EASI-90 to <EASI-100 vs. EASI-75 to <EASI-90 responders [200 mg: 67.6%, 48.9% vs. 28.8%; 100 mg: 63.2%, 48.1% vs. 36.7%]).
Conclusions: Substantial proportions of patients with moderate-to-severe AD receiving abrocitinib met higher threshold efficacy end points, and this was associated with meaningful additional QoL benefits compared with those who did not meet these higher efficacy thresholds. Not only do a substantial proportion of abrocitinib-treated patients achieve higher threshold efficacy end points but they also do so in a similar timeframe as the more commonly used thresholds for efficacy end points.
Clinical trials: NCT02780167, NCT03349060 and NCT03575871.
© 2022 Pfizer Inc. Journal of the European Academy of Dermatology and Venereology published by John Wiley & Sons Ltd on behalf of European Academy of Dermatology and Venereology.
Figures
References
-
- Silverberg JI, Hanifin JM. Adult eczema prevalence and associations with asthma and other health and demographic factors: a US population‐based study. J Allergy Clin Immunol 2013; 132: 1132–1138. - PubMed
-
- Williams H, Robertson C, Stewart A et al. Worldwide variations in the prevalence of symptoms of atopic eczema in the international study of asthma and allergies in childhood. J Allergy Clin Immunol 1999; 103: 125–138. - PubMed
-
- Chiesa Fuxench ZC, Block JK, Boguniewicz M et al. Atopic dermatitis in America study: a cross‐sectional study examining the prevalence and disease burden of atopic dermatitis in the US adult population. J Invest Dermatol 2019; 139: 583–590. - PubMed
-
- Silverberg JI, Gelfand JM, Margolis DJ et al. Patient burden and quality of life in atopic dermatitis in US adults: a population‐based cross‐sectional study. Ann Allergy Asthma Immunol 2018; 121: 340–347. - PubMed
-
- Thyssen JP, Andersen Y, Halling AS, Williams HC, Egeberg A. Strengths and limitations of the United Kingdom working party criteria for atopic dermatitis in adults. J Eur Acad Dermatol Venereol 2020; 34: 1764–1772. - PubMed
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
