

Archetypal Analysis of Injury in Kidney Transplant Biopsies Identifies Two Classes of Early AKI
- PMID: 35463013
- PMCID: PMC9021747
- DOI: 10.3389/fmed.2022.817324
Archetypal Analysis of Injury in Kidney Transplant Biopsies Identifies Two Classes of Early AKI
Abstract
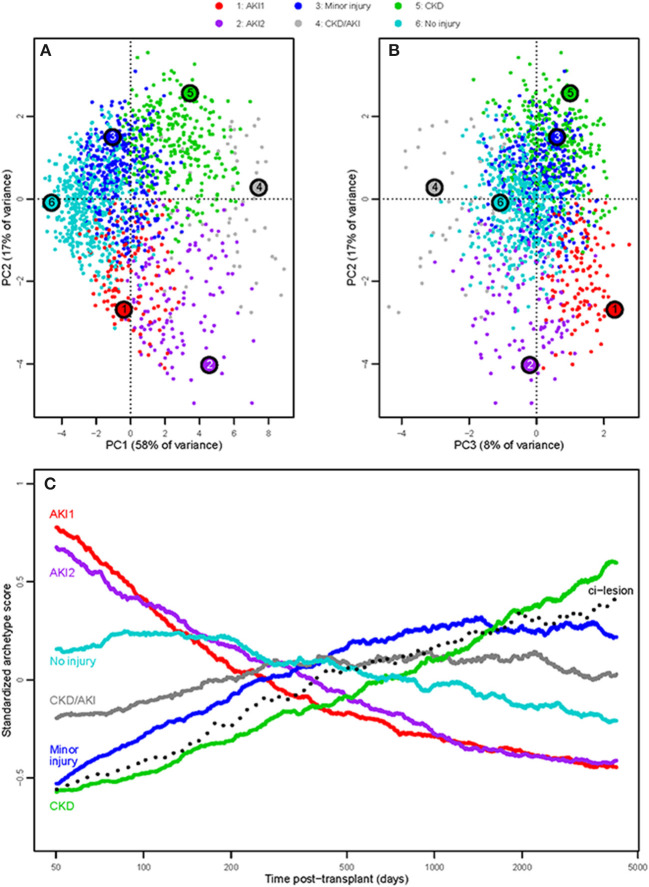
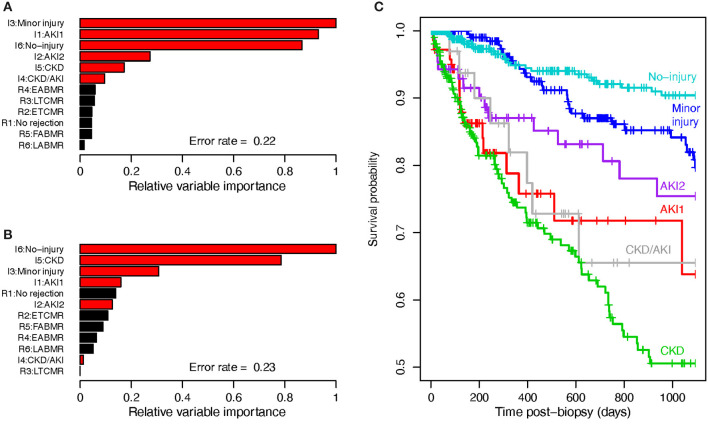
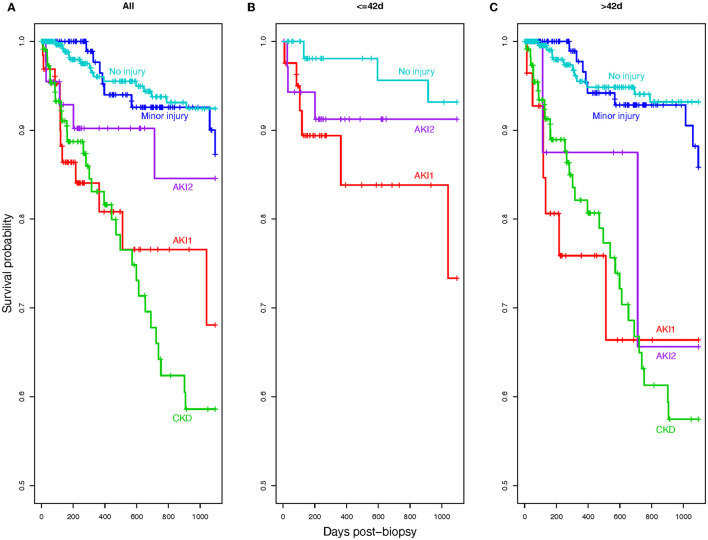
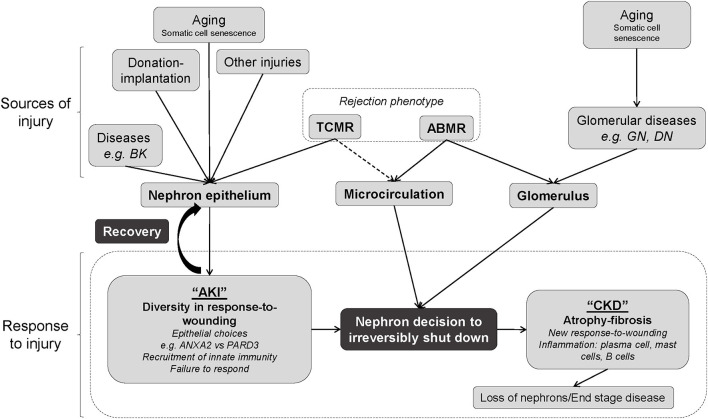
All transplanted kidneys are subjected to some degree of injury as a result of the donation-implantation process and various post-transplant stresses such as rejection. Because transplants are frequently biopsied, they present an opportunity to explore the full spectrum of kidney response-to-wounding from all causes. Defining parenchymal damage in transplanted organs is important for clinical management because it determines function and survival. In this study, we classified the scenarios associated with parenchymal injury in genome-wide microarray results from 1,526 kidney transplant indication biopsies collected during the INTERCOMEX study. We defined injury groups by using archetypal analysis (AA) of scores for gene sets and classifiers previously identified in various injury states. Six groups and their characteristics were defined in this population: No injury, minor injury, two classes of acute kidney injury ("AKI," AKI1, and AKI2), chronic kidney disease (CKD), and CKD combined with AKI. We compared the two classes of AKI, namely, AKI1 and AKI2. AKI1 had a poor function and increased parenchymal dedifferentiation but minimal response-to-injury and inflammation, instead having increased expression of PARD3, a gene previously characterized as being related to epithelial polarity and adherens junctions. In contrast, AKI2 had a poor function and increased response-to-injury, significant inflammation, and increased macrophage activity. In random forest analysis, the most important predictors of function (estimated glomerular filtration rate) and graft loss were injury-based molecular scores, not rejection scores. AKI1 and AKI2 differed in 3-year graft survival, with better survival in the AKI2 group. Thus, injury archetype analysis of injury-induced gene expression shows new heterogeneity in kidney response-to-wounding, revealing AKI1, a class of early transplants with a poor function but minimal inflammation or response to injury, a deviant response characterized as PC3, and an increased risk of failure. Given the relationship between parenchymal injury and kidney survival, further characterization of the injury phenotypes in kidney transplants will be important for an improved understanding that could have implications for understanding native kidney diseases (ClinicalTrials.gov #NCT01299168).
Keywords: archetypes; biopsy; gene expression; injury; kidney transplantation.
Copyright © 2022 Halloran, Böhmig, Bromberg, Einecke, Eskandary, Gupta, Myslak, Viklicky, Perkowska-Ptasinska, Madill-Thomsen and the INTERCOMEX Investigators.
Conflict of interest statement
PH is a consultant to Natera, holds shares in Transcriptome Sciences Inc (TSI), a University of Alberta research company dedicated to developing molecular diagnostics, supported in part by a licensing agreement between TSI and Thermo Fisher, and by a research grant from Natera. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Associated data
LinkOut - more resources
Full Text Sources
Medical