

Interactive Training of the Emergency Medical Services Improved Prehospital Stroke Recognition and Transport Time
- PMID: 35463146
- PMCID: PMC9021450
- DOI: 10.3389/fneur.2022.765165
Interactive Training of the Emergency Medical Services Improved Prehospital Stroke Recognition and Transport Time
Abstract
Background and purpose: Acute stroke treatment outcomes are predicated on reperfusion timeliness which can be improved by better prehospital stroke identification. We aimed to assess the effect of interactive emergency medical services (EMS) training on stroke recognition and prehospital care performance in a very high-risk cardiovascular risk population in Lithuania.
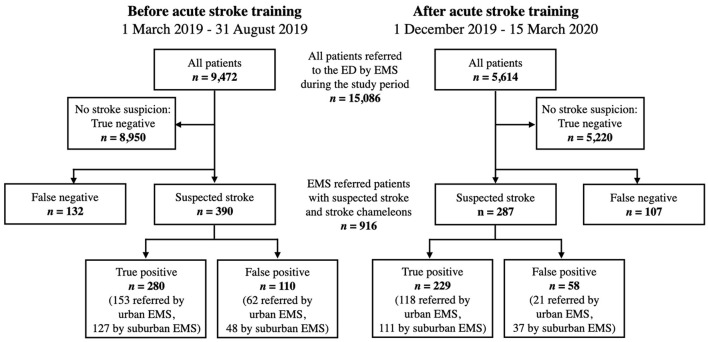
Methods: We conducted a single-center interrupted time-series study between March 1, 2019 and March 15, 2020. Two-hour small-group interactive stroke training sessions were organized for 166 paramedics serving our stroke network. We evaluated positive predictive value (PPV) and sensitivity for stroke including transient ischemic attack identification, onset-to-door time, and hospital-based outcomes during 6-months prior and 3.5 months after the training. The study outcomes were compared between EMS providers in urban and suburban areas.
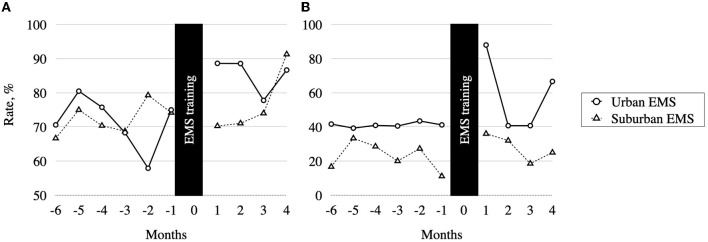
Results: In total, 677 suspected stroke cases and 239 stroke chameleons (median age 75 years, 54.8% women) were transported by EMS. After the training, we observed improved PPV for stroke recognition (79.8% vs. 71.8%, p = 0.017) and a trend of decreased in-hospital mortality (7.8% vs. 12.3, p = 0.070). Multivariable logistic regression models adjusted for age, gender, EMS location, and stroke subtype showed an association between EMS stroke training and improved odds of stroke identification (adjusted odds ratio [aOR] 1.6 [1.1-2.3]) and onset-to-door ≤ 90 min (aOR 1.6 [1.1-2.5]). The improvement of PPV was observed in urban EMS (84.9% vs. 71.2%, p = 0.003), but not in the suburban group (75.0% vs. 72.6%, p = 0.621).
Conclusions: The interactive EMS training was associated with a robust improvement of stroke recognition, onset to hospital transport time, and a trend of decreased in-hospital mortality. Adapted training strategies may be needed for EMS providers in suburban areas. Future studies should evaluate the long-term effects of the EMS training and identify optimal retraining intervals.
Keywords: emergency medical services (EMS); prehospital/EMS; stroke; training; transient ischemic attack (TIA); triage.
Copyright © 2022 Sveikata, Melaika, Wiśniewski, Vilionskis, Petrikonis, Stankevičius, Jurjans, Ekkert, Jatužis and Masiliūnas.
Conflict of interest statement
This study received funding from Boehringer Ingelheim GmbH & Co KG Lithuania. The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit for publication. The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources