

Predicting Bone Metastasis Risk Based on Skull Base Invasion in Locally Advanced Nasopharyngeal Carcinoma
- PMID: 35463321
- PMCID: PMC9022773
- DOI: 10.3389/fonc.2022.812358
Predicting Bone Metastasis Risk Based on Skull Base Invasion in Locally Advanced Nasopharyngeal Carcinoma
Abstract
Objective: To develop and validate a bone metastasis prediction model based on skull base invasion (SBI) in patients with locally advanced nasopharyngeal carcinoma (LA-NPC).
Methods: This retrospective cohort study enrolled 290 patients with LA-NPC who received intensity-modulated radiation therapy in two hospitals from 2010 to 2020. Patient characteristics were grouped by SBI and hospital. Both unadjusted and multivariate-adjusted models were used to determine bone metastasis risk based on SBI status. Subgroup analysis was performed to investigate heterogeneity using a forest graph. Cox proportional hazard regression analysis was used to screen for risk factors of bone metastasis-free survival (BMFS). A nomogram of BMFS based on SBI was developed and validated using C-index, receiver operating characteristic curve, calibration curves, and decision curve analysis after Cox proportional hazard regression analysis.
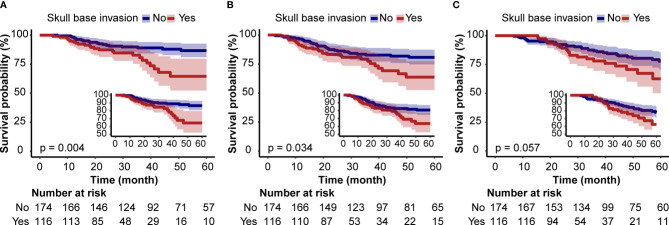
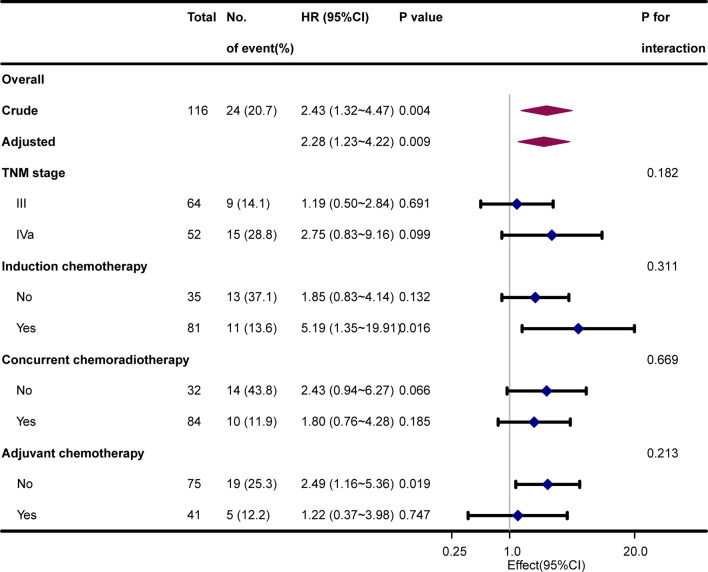
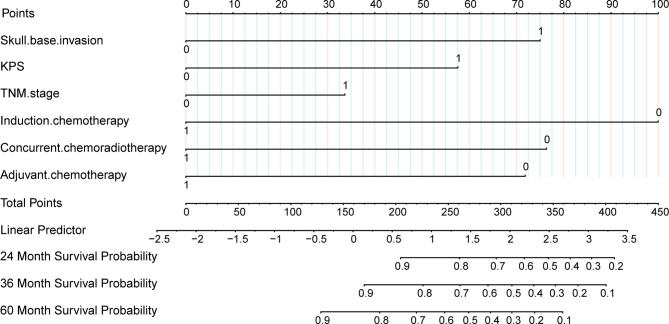
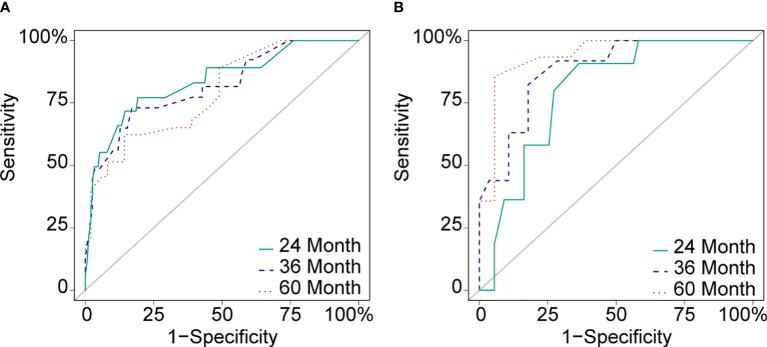
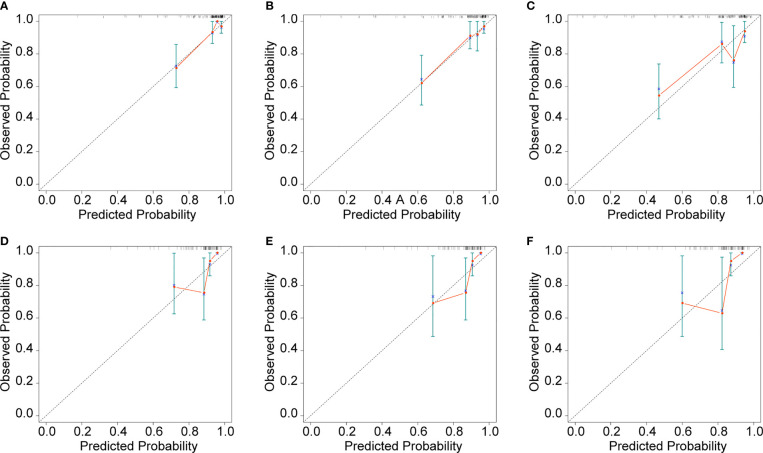
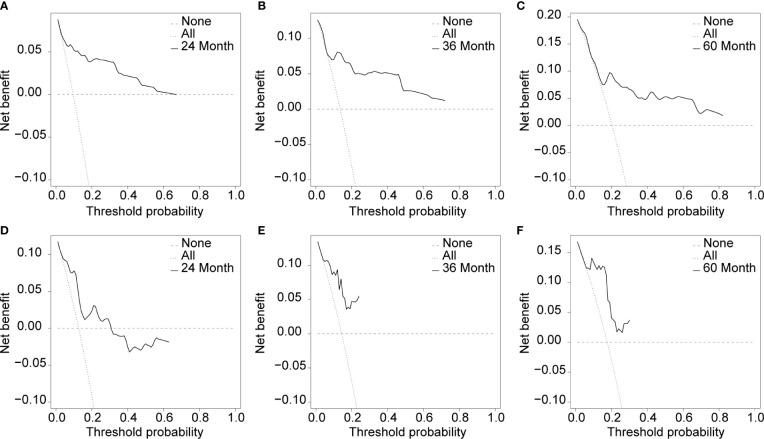
Results: The incidence of bone metastasis was 14.83% (43/290), 20.69% (24/116), and 10.92% (19/174) in the overall population, SBI-positive group, and SBI-negative group, respectively. In the unadjusted model, SBI was associated with reduced BMFS [HR 2.43 (1.32-4.47), P = 0.004], and the results remained stable after three continuous adjustments (P <0.05). No significant interaction was found in the subgroup analyses (P for interaction >0.05). According to Cox proportional hazard regression analysis and clinical value results, potential risk factors included SBI, Karnofsky performance status, TNM stage, induction chemotherapy, concurrent chemoradiotherapy, and adjuvant chemotherapy. Using a training C-index of 0.80 and a validation C-index of 0.79, the nomogram predicted BMFS and demonstrated satisfactory prognostic capability in 2, 3, and 5 years (area under curve: 83.7% vs. 79.6%, 81.7% vs. 88.2%, and 79.0% vs. 93.8%, respectively).
Conclusion: Skull base invasion is a risk factor for bone metastasis in patients with LA-NPC. The SBI-based nomogram model can be used to predict bone metastasis and may assist in identifying LA-NPC patients at the highest risk of bone metastasis.
Keywords: bone metastasis; bone metastasis-free survival; intensity modulated radiation therapy; nasopharyngeal carcinoma; nomogram; prediction model; skull base invasion.
Copyright © 2022 Wu, Guo, Yang, Gao and Tian.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Value of skull base invasion subclassification in nasopharyngeal carcinoma: implication for prognostic stratification and use of induction chemotherapy.Eur Radiol. 2022 Nov;32(11):7767-7777. doi: 10.1007/s00330-022-08864-7. Epub 2022 May 31. Eur Radiol. 2022. PMID: 35639144 Free PMC article.
-
Development of a Nomogram Model for Treatment of Nonmetastatic Nasopharyngeal Carcinoma.JAMA Netw Open. 2020 Dec 1;3(12):e2029882. doi: 10.1001/jamanetworkopen.2020.29882. JAMA Netw Open. 2020. PMID: 33306119 Free PMC article.
-
Establishment of a Prognostic Nomogram for Patients With Locoregionally Advanced Nasopharyngeal Carcinoma Incorporating TNM Stage, Post-Induction Chemotherapy Tumor Volume and Epstein-Barr Virus DNA Load.Front Oncol. 2021 Jun 16;11:683475. doi: 10.3389/fonc.2021.683475. eCollection 2021. Front Oncol. 2021. PMID: 34222003 Free PMC article.
-
Prognostic nomogram for patients with Nasopharyngeal Carcinoma incorporating hematological biomarkers and clinical characteristics.Int J Biol Sci. 2018 Apr 5;14(5):549-556. doi: 10.7150/ijbs.24374. eCollection 2018. Int J Biol Sci. 2018. PMID: 29805306 Free PMC article.
-
Meta-Analysis on Induction Chemotherapy in Locally Advanced Nasopharyngeal Carcinoma.Oncologist. 2021 Jan;26(1):e130-e141. doi: 10.1002/ONCO.13520. Epub 2020 Oct 1. Oncologist. 2021. PMID: 32924198 Free PMC article.
Cited by
-
U-shaped association between serum calcium and in-hospital mortality in patients with congestive heart failure.ESC Heart Fail. 2024 Oct;11(5):2521-2530. doi: 10.1002/ehf2.14730. Epub 2024 Mar 11. ESC Heart Fail. 2024. PMID: 38467491 Free PMC article.
-
The utility of texture analysis based on quantitative synthetic magnetic resonance imaging in nasopharyngeal carcinoma: a preliminary study.BMC Med Imaging. 2023 Jan 25;23(1):15. doi: 10.1186/s12880-023-00968-w. BMC Med Imaging. 2023. PMID: 36698156 Free PMC article.
-
The map of bone metastasis in nasopharyngeal carcinoma: A real-world study.Cancer Med. 2023 Sep;12(17):17660-17670. doi: 10.1002/cam4.6383. Epub 2023 Aug 10. Cancer Med. 2023. PMID: 37563937 Free PMC article.
-
J-Shaped Association Between Respiratory Rate and In-Hospital Mortality in Acute Myocardial Infarction Patients Complicated by Congestive Heart Failure in Intensive Care Unit.Dose Response. 2024 Dec 2;22(4):15593258241303040. doi: 10.1177/15593258241303040. eCollection 2024 Oct-Dec. Dose Response. 2024. PMID: 39629219 Free PMC article.
-
Deep learning model using planar whole-body bone scintigraphy for diagnosis of skull base invasion in patients with nasopharyngeal carcinoma.J Cancer Res Clin Oncol. 2024 Oct 9;150(10):449. doi: 10.1007/s00432-024-05969-y. J Cancer Res Clin Oncol. 2024. PMID: 39379746 Free PMC article.
References
-
- Ji MF, Sheng W, Cheng WM, Ng MH, Wu BH, Yu X, et al. . Incidence and Mortality of Nasopharyngeal Carcinoma: Interim Analysis of a Cluster Randomized Controlled Screening Trial (PRO-NPC-001) in Southern China. Ann Oncol: Off J Eur Soc Med Oncol (2019) 30(10):1630–7. doi: 10.1093/annonc/mdz231 - DOI - PubMed
LinkOut - more resources
Full Text Sources