

Percentage of Tumor Invasion at Pretreatment High-Resolution Magnetic Resonance Imaging: Associating With Aggressive and Tumor Response in Chinese T3 Rectal Cancer-Preliminary Results
- PMID: 35463367
- PMCID: PMC9021692
- DOI: 10.3389/fonc.2022.616310
Percentage of Tumor Invasion at Pretreatment High-Resolution Magnetic Resonance Imaging: Associating With Aggressive and Tumor Response in Chinese T3 Rectal Cancer-Preliminary Results
Abstract
Purpose: The purpose of the study was to assess the ability of percentage of tumor invasion (PTI) of T3 rectal cancer on pretreatment MRI as an imaging biomarker to reflect aggressiveness and to predict tumor response after neoadjuvant chemoradiation (NCRT) in Chinese population.
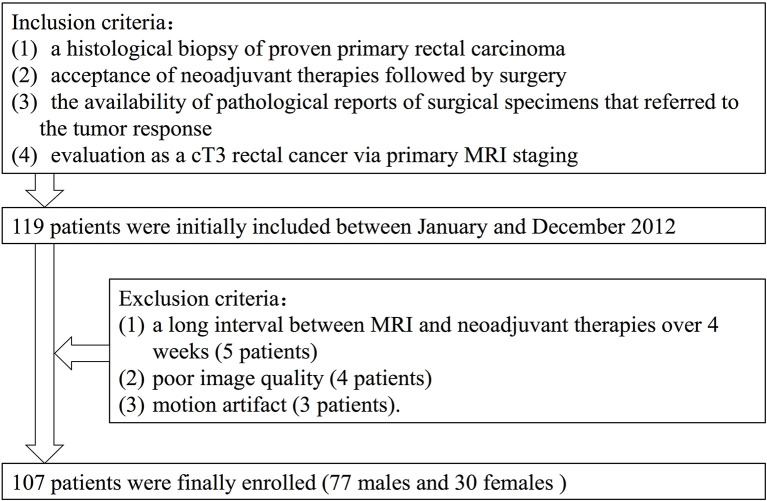
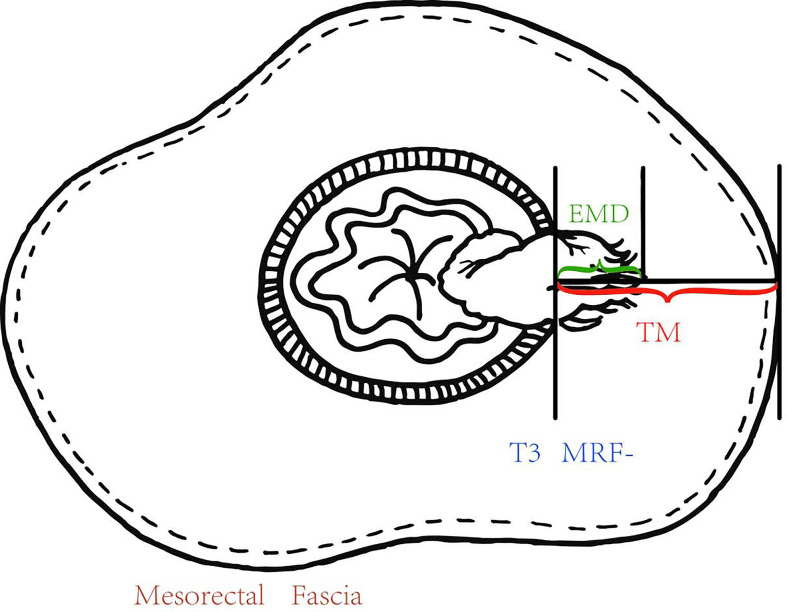
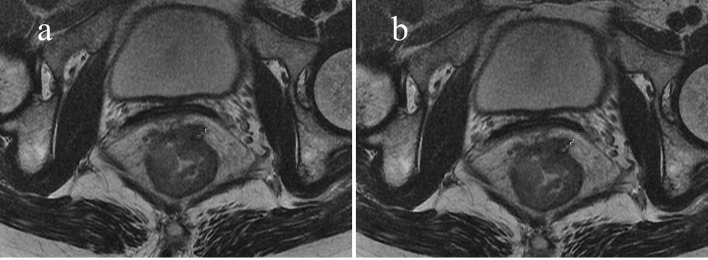
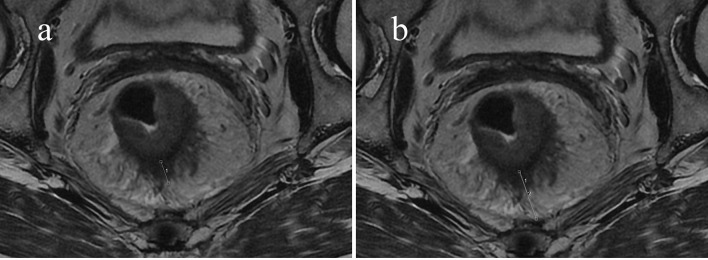
Methods: A total of 107 Chinese rectal cancer patients who underwent pretreatment MRI staging as T3 were included. The extramural depth of tumor invasion (EMD), the distance between outer border of muscularis propria (MP) and mesorectal fascia (MRF) we called "thickness of the mesorectum (TM)") at the same slice and direction were measured at pretreatment MRI, and PTI was equal to EMD/TM, was calculated. The EMD and PTI of subgroups based on pretreatment CEA, CA19-9 levels; N category and pathological complete response (pCR) were compared. The parameters, which described tumor invasion, were compared between pCR and non-pCR group. Student t-tests and logistic analysis were applied.
Results: The pretreatment PTI was higher in CEA ≥5.2 ng/ml patients (58.52% ± 27.68%) than in CEA <5.2 ng/ml patients (47.27% ± 24.15%) (p = 0.034). The pretreatment EMD in non-pCR group (7.21 ± 2.85 mm) was higher than in pCR group (6.14 ± 3.56 mm) (p = 0.049). The pretreatment PTI in non-pCR group (57.4% ± 26.4%) was higher than in pCR group (47.3% ± 29.1%) (p = 0.041). Compared with patients with PTI ≥50%, MRF (+), more patients with PTI <50%, MRF (-) showed pCR (OR = 8.44, p = 0.005; OR = 6.32, p = 0.024).
Conclusion: The PTI obtained at pretreatment MRI may serve as an imaging biomarker to reflect tumor aggressiveness and predict which T3 rectal cancer patients may benefit from NCRT in Chinese population.
Keywords: chemoradiotherapy; feasibility studies; magnetic resonance imaging; neoplasm staging; rectal neoplasms.
Copyright © 2022 Hu, Li, Sun, Sun and Tong.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Taylor FG, Quirke P, Heald RJ, Moran B, Blomqvist L, Swift I, et al. MERCURY Study Group. Preoperative High- Resolution Magnetic Resonance Imaging can Identify Good Prognosis Stage I, II, and III Rectal Cancer Best Managed by Surgery Alone: A Prospective, Multicenter,European Study. Ann Surg (2011) 253:711–9. doi: 10.1097/SLA.0b013e31820b8d52 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous