

Aortic root widening: "pro et contra"
- PMID: 35463701
- PMCID: PMC8980977
- DOI: 10.1007/s12055-020-01125-6
Aortic root widening: "pro et contra"
Abstract
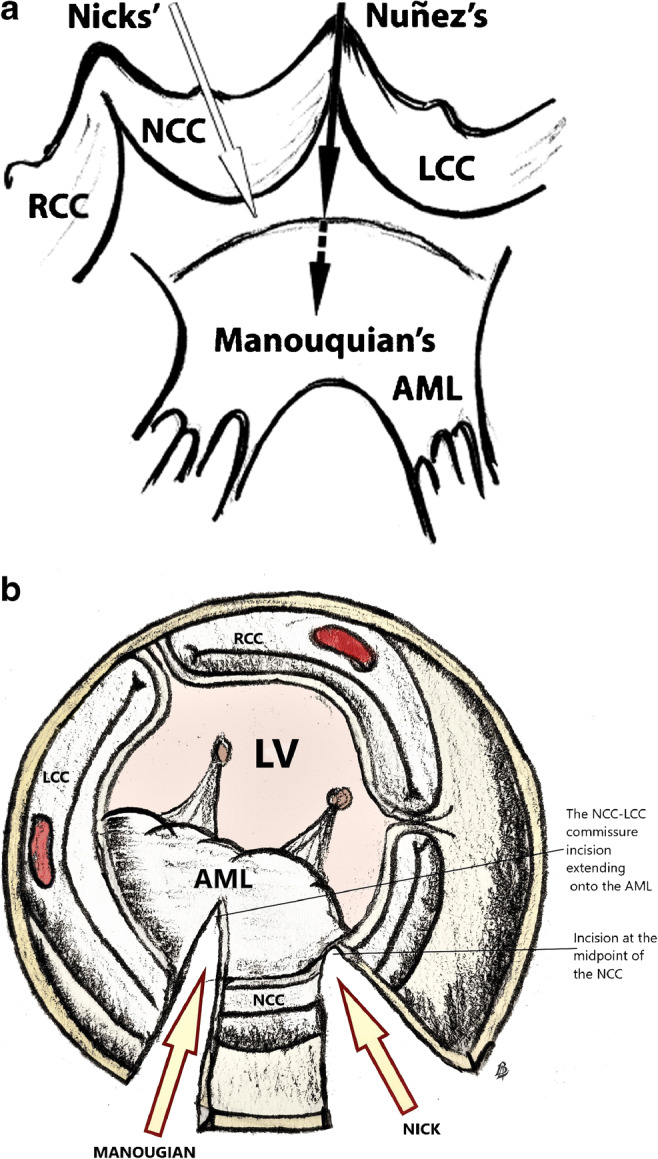
In patients with a small aortic annulus, the clinical benefits of aortic valve replacement depend on avoidance of patient-prosthesis mismatch as it is associated with reduced overall survival. Aortic root widening or enlargement is a useful technique to implant larger valve prosthesis to prevent patient-prosthesis mismatch. Posterior annular enlargement is the commonest technique used for aortic root enlargement. Consistent enlargement of the aortic root requires more extensive procedures like Manouguian or Konno-Rastan techniques. The patients commonly selected are younger patients with good life expectancy. However, caution is advised in applying this procedure in elderly patients, patients with heavily calcified annulus and when performing concomitant procedures. There is no definitive conclusion on the best material to use for the reconstruction of aortic annulus and aorta in aortic root enlargement procedures.
Keywords: Aortic root enlargement; Aortic valve stenosis; Manouguian; Nicks; Patient-prosthesis mismatch.
© Indian Association of Cardiovascular-Thoracic Surgeons 2021.
Conflict of interest statement
Conflict of interestThe authors declare that they have no conflicts of interest.
Figures






References
-
- Horstkotte D, Loogen F. The natural history of aortic valve stenosis. Eur Heart J. 1988;9:57–64. - PubMed
-
- Nishimura RA, Otto CM, Bonow RO, et al. 2014 AHA/ACC guideline for the management of patients with valvular heart disease: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129:2440–2492. - PubMed
-
- Chambers J. Echocardiography and the small aortic root. J Heart Valve Dis. 1996;5:S264–S268. - PubMed
-
- Ghosh P, Kumar S, Pandey S, Kumar AS, Sinha N. Small aortic annulus: a functional definition. Ann Thorac Cardiovasc Surg. 1998;4:251–261. - PubMed
-
- Freitas-Ferraz AB, Tirado-Conte G, Dagenais F, et al. Aortic stenosis and small aortic annulus. Circulation. 2019;139:2685–2702. - PubMed
LinkOut - more resources
Full Text Sources