

Association of anti-neutrophil cytoplasmic antibody-associated vasculitis and cardiovascular events: a population-based cohort study
- PMID: 35464192
- PMCID: PMC9022464
- DOI: 10.1093/ckj/sfab229
Association of anti-neutrophil cytoplasmic antibody-associated vasculitis and cardiovascular events: a population-based cohort study
Abstract
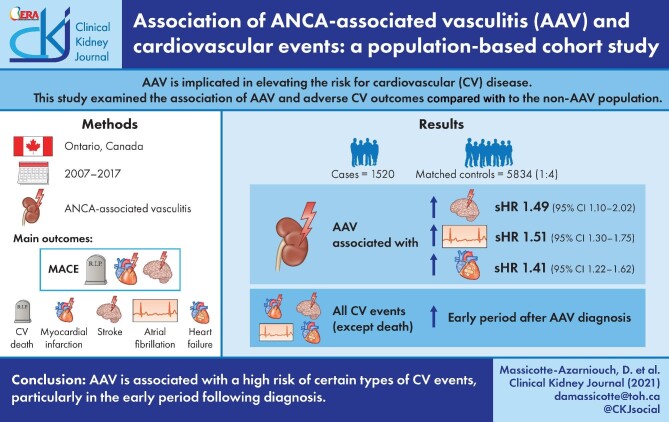
Background: Anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV) is implicated in elevating the risk for cardiovascular (CV) disease; whether the elevated risk applies to all types of CV diseases or specific types is unclear. This study examined the association of AAV and adverse CV outcomes compared with the non-AAV population.
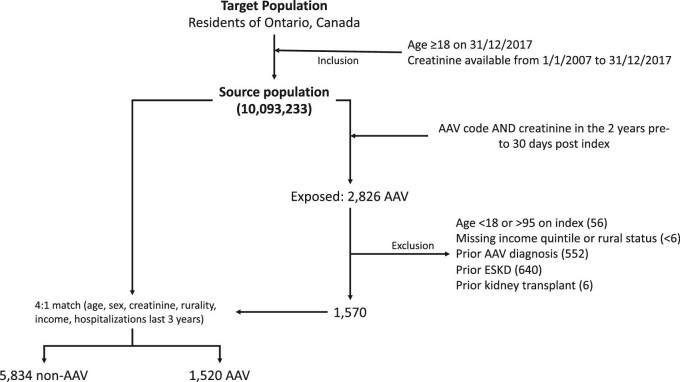
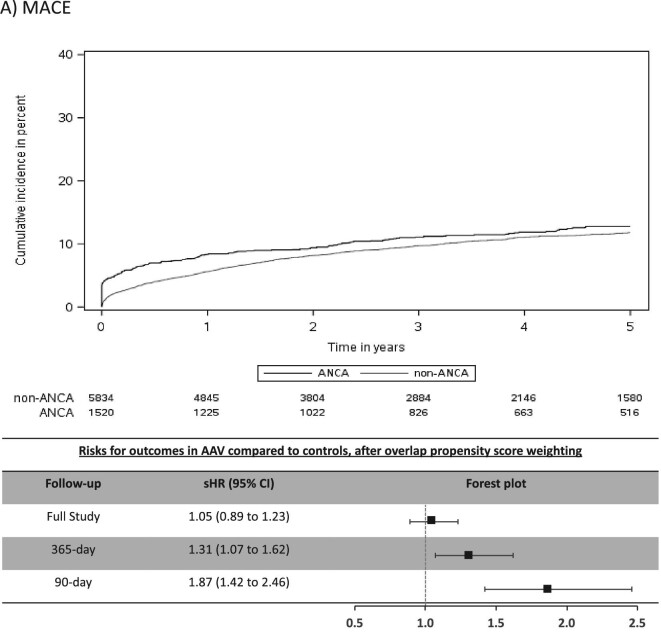
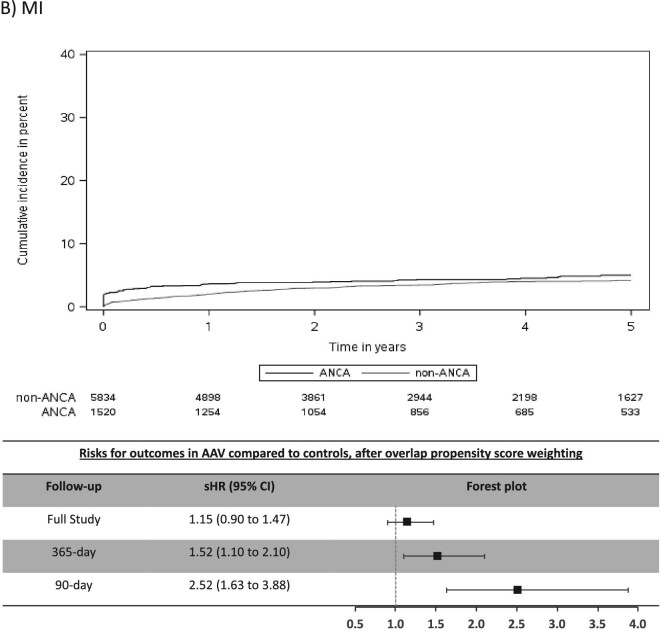
Methods: We conducted a population-based, retrospective cohort study of adults (mean age 61 years, 51% female) with a new diagnosis of AAV in Ontario, Canada from 2007 to 2017. Weighted models were used to examine the association of AAV (n = 1520) and CV events in a matched (1:4) control cohort (n = 5834). The main outcomes were major adverse CV events (MACE), defined as myocardial infarction (MI), stroke or CV death, its components, atrial fibrillation (AF) and congestive heart failure (CHF).
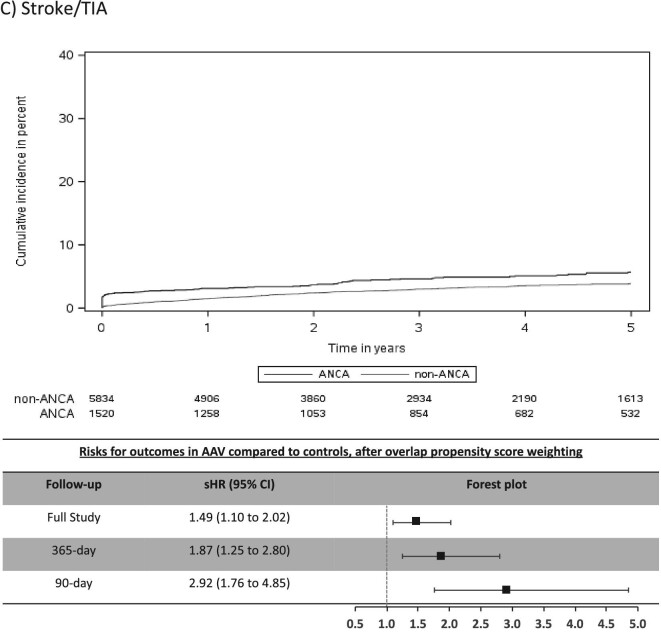
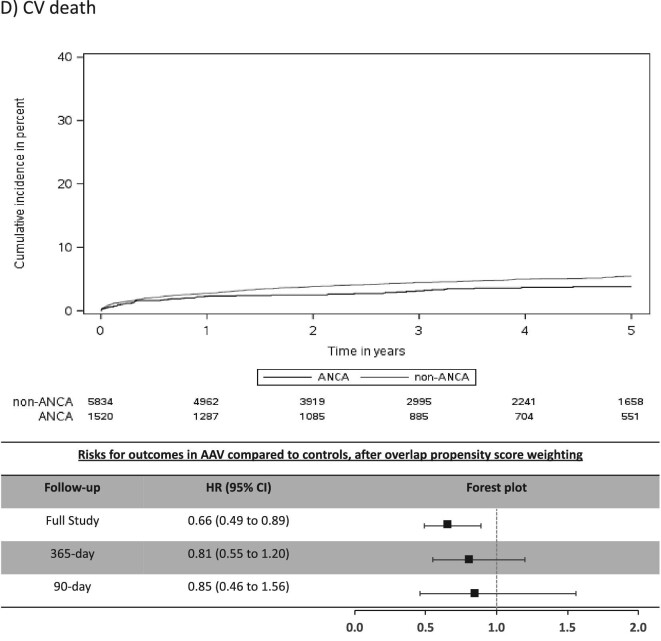
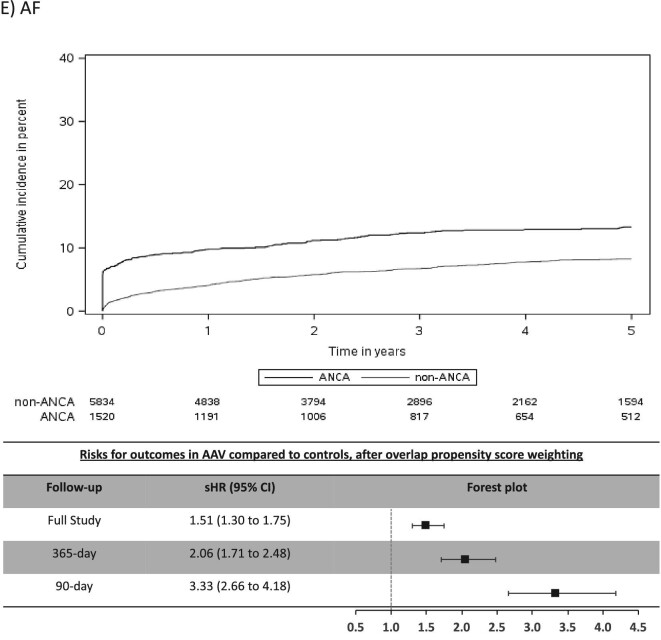
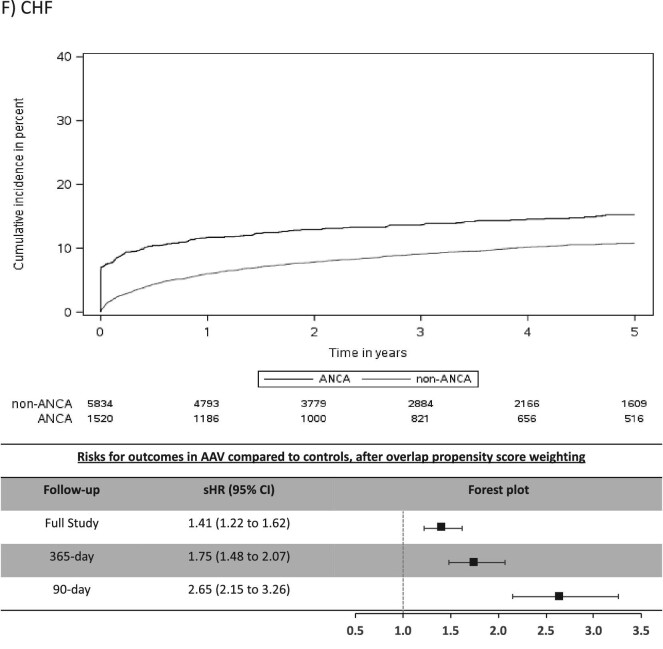
Results: Over a mean follow-up of 3.8 years, AAV (compared with non-AAV) was associated with a higher risk of stroke: cumulative incidence 7.0% versus 5.2%, sub-distribution hazard ratio (sHR) 1.49 [(95% confidence interval (95% CI) 1.10-2.02]; AF: cumulative incidence 16.4% versus 11.5%, sHR 1.51, 95% CI 1.30-1.75; and CHF: cumulative incidence 20.8% versus 13.3%, sHR 1.41, 95% CI 1.22-1.62; but not for MACE, MI or CV death. The risks for all CV events, except CV death, were significantly elevated in the early period after AAV diagnosis, in particular AF (365-day sHR 2.06, 95% CI 1.71-2.48; 90-day sHR 3.33, 95% CI 2.66-4.18) and CHF (365-day sHR 1.75, 95% CI 1.48-2.07; 90-day sHR 2.65, 95% CI 2.15-3.26).
Conclusion: AAV is associated with a high risk of certain types of CV events, particularly in the early period following diagnosis.
Keywords: ANCA-associated vasculitis; atrial fibrillation; cardiovascular events; congestive heart failure.
© The Author(s) 2021. Published by Oxford University Press on behalf of the ERA.
Figures
Comment on
-
Cardiovascular disease and ANCA-associated vasculitis: are we missing a beat?Clin Kidney J. 2022 Jan 13;15(4):618-623. doi: 10.1093/ckj/sfac009. eCollection 2022 Apr. Clin Kidney J. 2022. PMID: 35371453 Free PMC article.
References
-
- Jennette JC, Falk RJ, Bacon PAet al. . 2012 Revised international Chapel Hill consensus conference nomenclature of vasculitides. Arthritis Rheum 2013; 65: 1–11 - PubMed
-
- De Groot K, Harper L, Jayne DRWet al. . Pulse versus daily oral cyclophosphamide for induction of remission in antineutrophil cytoplasmic antibody-associated vasculitis: a randomized trial. Ann Intern Med 2009; 150: 670. - PubMed
-
- Jones RB, Cohen Tervaert JW, Hauser Tet al. . Rituximab versus cyclophosphamide in ANCA-associated renal vasculitis. N Engl J Med 2010; 363: 211–220 - PubMed
-
- Robson J, Doll H, Suppiah Ret al. . Damage in the ANCA-associated vasculitides: long-term data from the European vasculitis study group (EUVAS) therapeutic trials. Ann Rheum Dis 2015; 74: 177–184 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
