

Differences in SARS-CoV-2 Vaccine Response Dynamics Between Class-I- and Class-II-Specific T-Cell Receptors in Inflammatory Bowel Disease
- PMID: 35464463
- PMCID: PMC9024211
- DOI: 10.3389/fimmu.2022.880190
Differences in SARS-CoV-2 Vaccine Response Dynamics Between Class-I- and Class-II-Specific T-Cell Receptors in Inflammatory Bowel Disease
Abstract
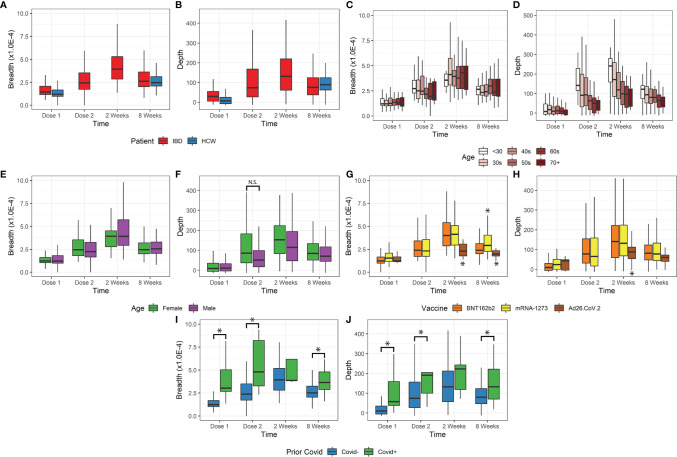
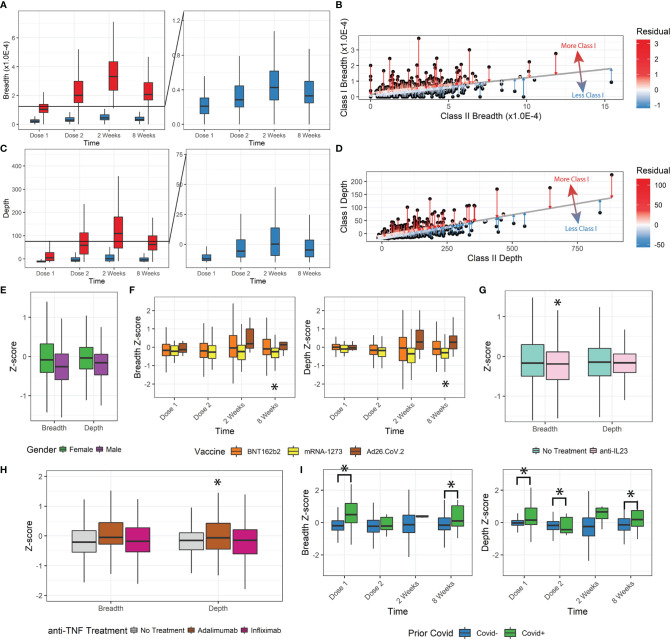
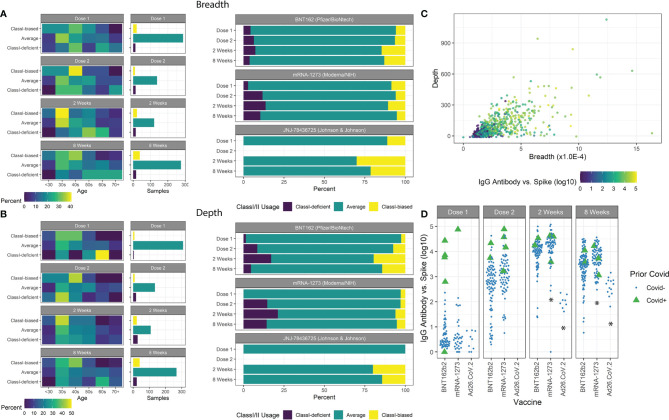
T-cells specifically bind antigens to induce adaptive immune responses using highly specific molecular recognition, and a diverse T-cell repertoire with expansion of antigen-specific clones can indicate robust immune responses after infection or vaccination. For patients with inflammatory bowel disease (IBD), a spectrum of chronic intestinal inflammatory diseases usually requiring immunomodulatory treatment, the T-cell response has not been well characterized. Understanding the patient factors that result in strong vaccination responses is critical to guiding vaccination schedules and identifying mechanisms of T-cell responses in IBD and other immune-mediated conditions. Here we used T-cell receptor sequencing to show that T-cell responses in an IBD cohort were influenced by demographic and immune factors, relative to a control cohort of health care workers (HCWs). Subjects were sampled at the time of SARS-CoV-2 vaccination, and longitudinally afterwards; TCR Vβ gene repertoires were sequenced and analyzed for COVID-19-specific clones. We observed significant differences in the overall strength of the T-cell response by age and vaccine type. We further stratified the T-cell response into Class-I- and Class-II-specific responses, showing that Ad26.COV2.S vector vaccine induced Class-I-biased T-cell responses, whereas mRNA vaccine types led to different responses, with mRNA-1273 vaccine inducing a more Class-I-deficient T-cell response compared to BNT162b2. Finally, we showed that these T-cell patterns were consistent with antibody levels from the same patients. Our results account for the surprising success of vaccination in nominally immuno-compromised IBD patients, while suggesting that a subset of IBD patients prone to deficiencies in T-cell response may warrant enhanced booster protocols.
Keywords: SARS-CoV-2 (COVID-19); T-cell repertoire; immunodeficiency; inflammatory bowel disease; mRNA vaccine.
Copyright © 2022 Xu, Li, Ebinger, Mengesha, Elyanow, Gittelman, Chapman, Joung, Botwin, Pozdnyakova, Debbas, Mujukian, Prostko, Frias, Stewart, Horizon, Merin, Sobhani, Figueiredo, Cheng, Kaplan, McGovern, Merchant, Melmed and Braun.
Conflict of interest statement
GM has consulted for AbbVie, Arena Pharmaceuticals, Boehringer-Ingelheim, Bristol-Meyers Squibb/Celgene, Entasis, Janssen, Medtronic, Pfizer, Samsung Bioepis, Shionogi, Takeda, Techlab, and has received research funding from Pfizer for an unrelated investigator-initiated study. JB has received research funding from Janssen. DM has consulted for Takeda, Boehringer-Ingelheim, Palatin Technologies, Bridge Biotherapeutics, Pfizer, and Gilead, and is a consultant/stockholder for Prometheus Biosciences. RE, RG, HC, and IK are employees of Adaptive Biotechnologies. JP, EF, and JS are employees of Abbott. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous