

Respiratory Interventions for Preterm Infants in LMICs: A Prospective Study From Cape Town, South Africa
- PMID: 35464776
- PMCID: PMC9019119
- DOI: 10.3389/fgwh.2022.817817
Respiratory Interventions for Preterm Infants in LMICs: A Prospective Study From Cape Town, South Africa
Abstract
Background: Preterm birth is a global public health issue and complications of preterm birth result in the death of approximately 1 million infants each year, 99% of which are in low-and-middle income countries (LMIC). Although respiratory interventions such as continuous positive airway pressure (CPAP) and surfactant have been shown to improve the outcomes of preterm infants with respiratory distress, they are not readily available in low-resourced areas. The aim of this study was to report the respiratory support needs and outcomes of preterm infants in a low-resourced setting, and to estimate the impact of a lack of access to these interventions on neonatal mortality.
Methods: We conducted a six-month prospective observational study on preterm infants <1,801 g admitted at Groote Schuur Hospital and Mowbray Maternity Hospital neonatal units in Cape Town, South Africa. We extrapolated results from the study to model the potential outcomes of these infants in the absence of these interventions.
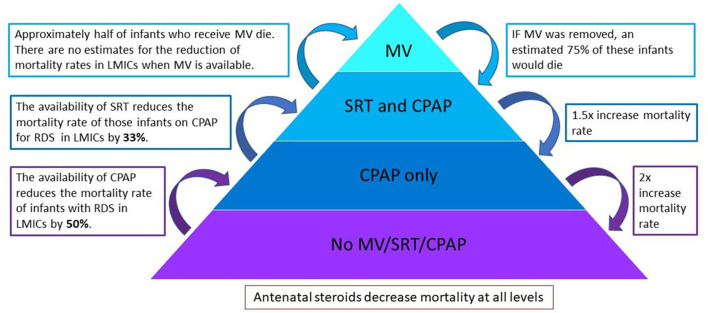
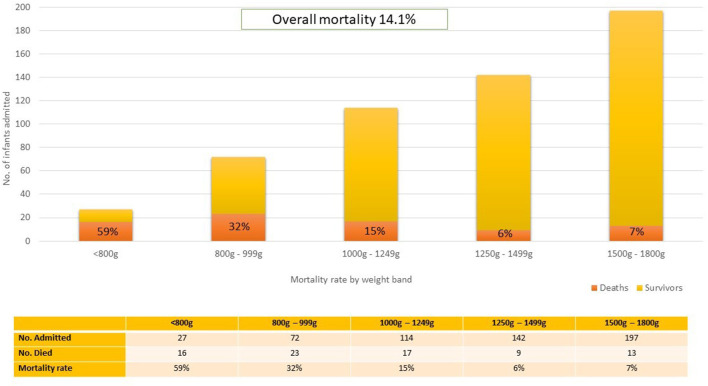
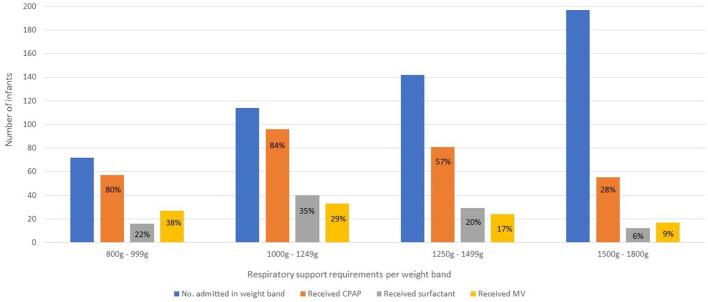
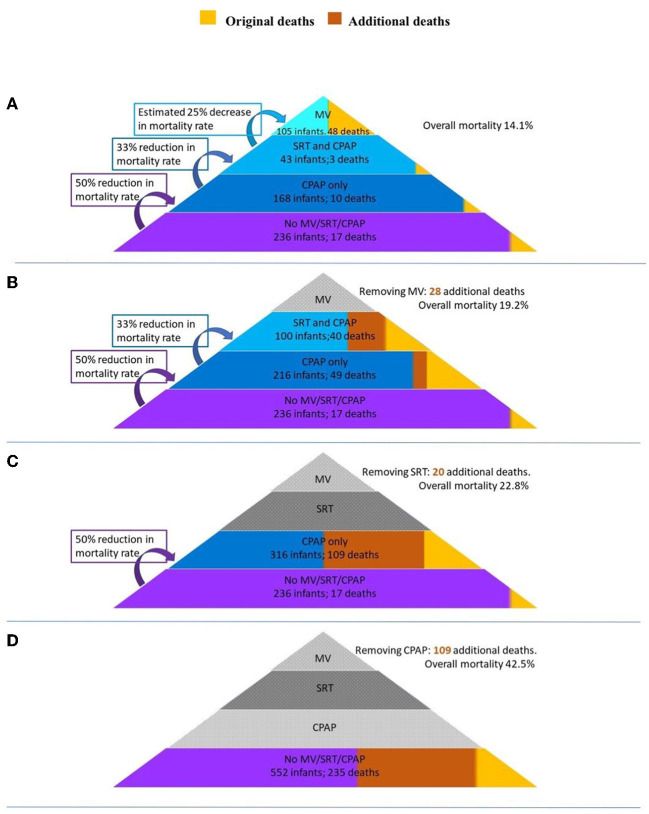
Results: Five hundred and fifty-two infants (552) <1,801 g were admitted. Three hundred (54.3%) infants received CPAP, and this was the initial respiratory intervention for most cases of respiratory distress syndrome. Surfactant was given to 100 (18.1%) infants and a less invasive method was the most common method of administration. Invasive mechanical ventilation was offered to 105 (19%) infants, of which only 57 (54.2%) survived until discharge from hospital. The overall mortality of the cohort was 14.1% and the hypothetical removal of invasive mechanical ventilation, surfactant and CPAP would result in an additional 157 deaths and increase the overall mortality to 42.5%. A lack of CPAP availability would have the largest impact on mortality and result in the largest number of additional deaths (109).
Conclusion: This study highlights the effect that access to key respiratory interventions has on preterm outcomes in LMICs. CPAP has the largest impact on neonatal mortality and improving its coverage should be the primary goal for low-resourced areas to save newborn lives.
Keywords: continuous positive airway pressure (CPAP); interventions; invasive mechanical ventilation; low-and-middle income countries (LMIC); preterm (birth); respiratory; respiratory distress syndrome (RDS); surfactant.
Copyright © 2022 Lategan, Price, Rhoda, Zar and Tooke.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
[Failure of non-invasive continuous positive airway pressure as the initial respiratory support in very preterm infants: a multicenter prospective cohort study].Zhonghua Er Ke Za Zhi. 2021 Apr 2;59(4):273-279. doi: 10.3760/cma.j.cn112140-20201117-01034. Zhonghua Er Ke Za Zhi. 2021. PMID: 33775045 Chinese.
-
Early nasal continuous positive airway pressure failure prediction in preterm infants less than 32 weeks gestational age suffering from respiratory distress syndrome.Pediatr Pulmonol. 2021 Dec;56(12):3879-3886. doi: 10.1002/ppul.25678. Epub 2021 Oct 5. Pediatr Pulmonol. 2021. PMID: 34610212
-
Study protocol for the POPART study-Prophylactic Oropharyngeal surfactant for Preterm infants: A Randomised Trial.BMJ Open. 2020 Jul 20;10(7):e035994. doi: 10.1136/bmjopen-2019-035994. BMJ Open. 2020. PMID: 32690739 Free PMC article.
-
Interventions for the Management of Respiratory Distress in Late Preterm and Term Infants Experiencing Delayed Respiratory Transition: A Systematic Review.Dimens Crit Care Nurs. 2019 Jul/Aug;38(4):192-200. doi: 10.1097/DCC.0000000000000365. Dimens Crit Care Nurs. 2019. PMID: 31145165
-
Non-invasive respiratory support for infants in low- and middle-income countries.Semin Fetal Neonatal Med. 2016 Jun;21(3):181-8. doi: 10.1016/j.siny.2016.02.003. Epub 2016 Feb 22. Semin Fetal Neonatal Med. 2016. PMID: 26915655 Review.
Cited by
-
Evaluation of a Novel Dry Powder Surfactant Aerosol Delivery System for Use in Premature Infants Supported with Bubble CPAP.Pharmaceutics. 2023 Sep 22;15(10):2368. doi: 10.3390/pharmaceutics15102368. Pharmaceutics. 2023. PMID: 37896128 Free PMC article.
-
Factors influencing survival and short-term outcomes of very low birth weight infants in a tertiary hospital in Johannesburg.Front Pediatr. 2022 Sep 16;10:930338. doi: 10.3389/fped.2022.930338. eCollection 2022. Front Pediatr. 2022. PMID: 36186656 Free PMC article.
-
Improving the Treatment of Neonatal Sepsis in Resource-Limited Settings: Gaps and Recommendations.Res Rep Trop Med. 2023 Dec 14;14:121-134. doi: 10.2147/RRTM.S410785. eCollection 2023. Res Rep Trop Med. 2023. PMID: 38116466 Free PMC article. Review.
-
Moving on from clinical animal-derived surfactants to peptide-based synthetic pulmonary surfactant.Am J Physiol Lung Cell Mol Physiol. 2024 Dec 1;327(6):L883-L889. doi: 10.1152/ajplung.00186.2024. Epub 2024 Oct 15. Am J Physiol Lung Cell Mol Physiol. 2024. PMID: 39404798 Free PMC article. Review.
References
-
- Perin J, Mulick A, Yeung D, Villavicencio F, Lopez G, Strong KL, et al. . Global, regional, and national causes of under-5 mortality in 2000–19: an updated systematic analysis with implications for the Sustainable Development Goals. Lancet Child Adolesc Health. (2022) 6:106-15. 10.1016/S2352-4642(21)00311-4 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources