

Posterior cerebral artery dissection after excessive caffeine consumption in a teenager
- PMID: 35464799
- PMCID: PMC9018804
- DOI: 10.1016/j.radcr.2022.02.035
Posterior cerebral artery dissection after excessive caffeine consumption in a teenager
Abstract
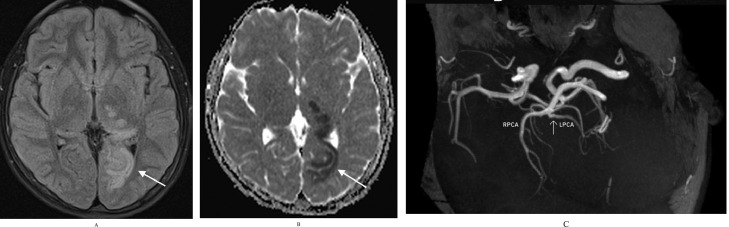
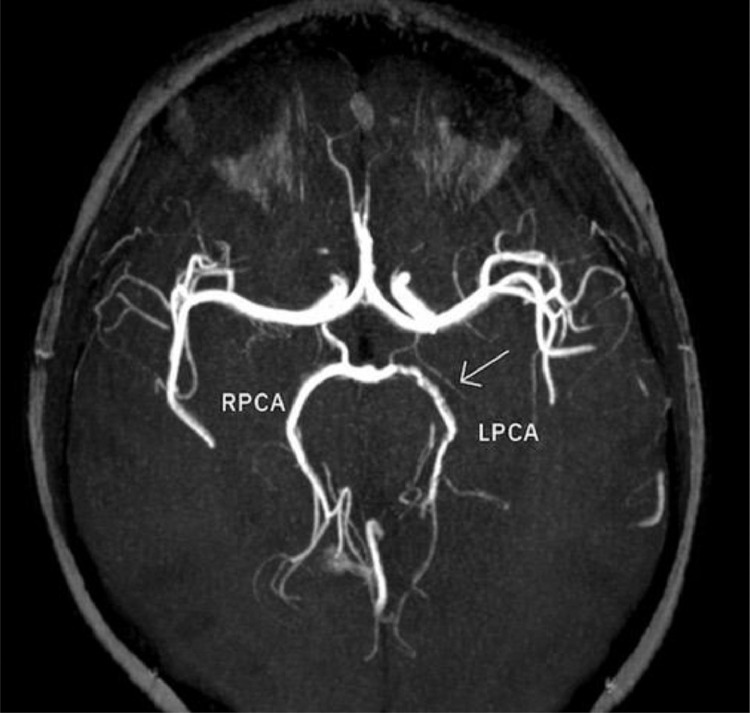
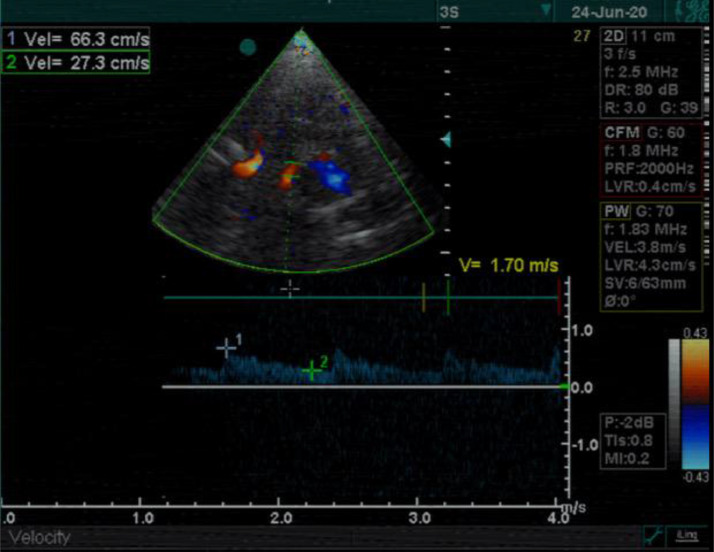
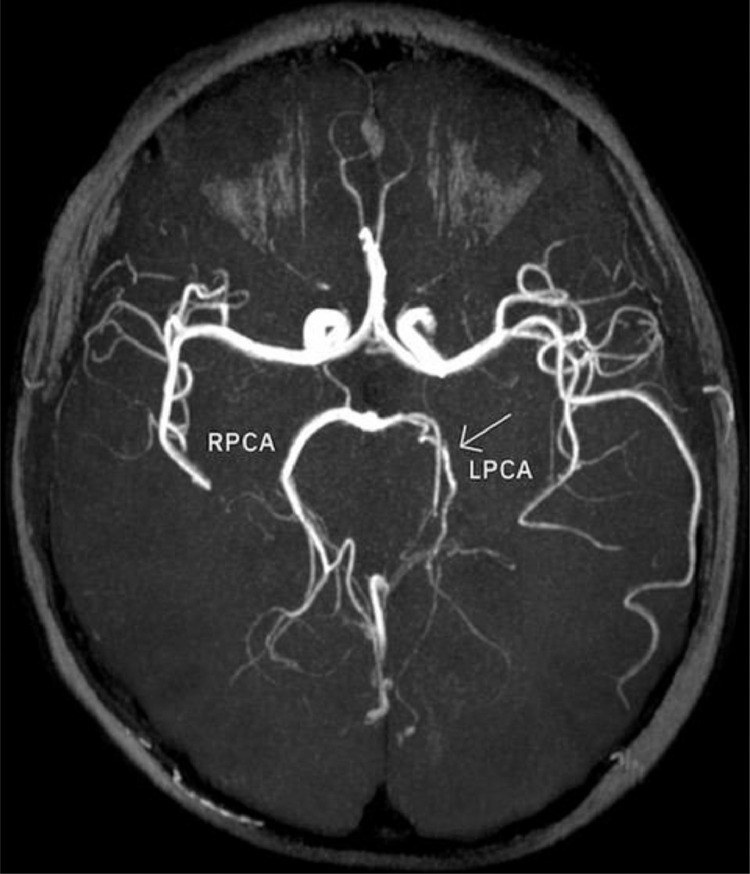
Arterial ischemic stroke is a rare but significant cause of neurological deficits in childhood. Even though there is a variety of risk factors, identifying the etiology can sometimes be a hard diagnostic challenge. Arteriopathies in general, and more specifically, arterial dissection is one of the uncommon pathologies that can cause incidents of pediatric stroke. We report a rare case of a young adolescent with posterior cerebral artery dissection after excessive consumption of caffeine, contained in energy drinks, only hours before the onset of neurological symptoms. A complete neuroimaging evaluation (MRI, intracranial US and digital subtraction angiography) at the admission and during the follow-ups supported the diagnosis of arterial dissection possibly caused by caffeine overconsumption.
Keywords: Caffeine; Dissection; Pediatric stroke; Posterior cerebral artery.
© 2022 The Authors.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources
