

A case of tongue cancer manifesting from oral leukoplakia after long-term administration of pegylated liposomal doxorubicin
- PMID: 35464897
- PMCID: PMC9021965
- DOI: 10.1093/omcr/omac042
A case of tongue cancer manifesting from oral leukoplakia after long-term administration of pegylated liposomal doxorubicin
Abstract
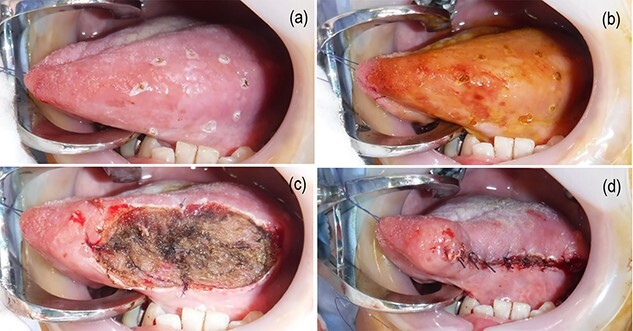
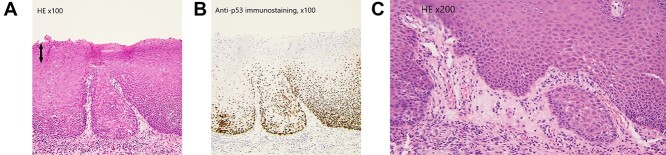
We present a case of tongue cancer manifestation from oral leukoplakia after administration of pegylated liposomal doxorubicin (PLD). A 56-year-old woman was diagnosed with ovarian cancer. After preoperative chemotherapy with paclitaxel and carboplatin (TC), she underwent interval debulking surgery. Five cycles of TC therapy were carried out as adjuvant chemotherapy; however, recurrence was observed. Despite administration of gemcitabine-carboplatin therapy, the patient's condition was judged as advancing to a progressive disease. PLD treatment was completed at a total dose of 1140 mg/m2. Two months after the end of treatment, the patient was diagnosed with leukoplakia. The leukoplakia lesion became thicker at each 3-month follow-up. She was diagnosed with tongue cancer and underwent a partial resection 2 years and 3 months after the completion of PLD treatment. Our report suggests that the risk of malignant transformation to tongue cancer persists even after the completion of treatment with PLD.
© The Author(s) 2022. Published by Oxford University Press. All rights reserved. For Permissions, please email: journals.permissions@oup.com.
Figures
Similar articles
-
Pegylated liposomal doxorubicin/carboplatin combination in ovarian cancer, progressing on single-agent pegylated liposomal doxorubicin.World J Clin Oncol. 2012 Oct 10;3(10):137-41. doi: 10.5306/wjco.v3.i10.137. World J Clin Oncol. 2012. PMID: 23198277 Free PMC article.
-
Carboplatin plus paclitaxel versus carboplatin plus pegylated liposomal doxorubicin as first-line treatment for patients with ovarian cancer: the MITO-2 randomized phase III trial.J Clin Oncol. 2011 Sep 20;29(27):3628-35. doi: 10.1200/JCO.2010.33.8566. Epub 2011 Aug 15. J Clin Oncol. 2011. PMID: 21844495 Clinical Trial.
-
Efficacy of pegylated liposomal doxorubicin (PLD) plus carboplatin in ovarian cancer patients who recur within six to twelve months: a phase II study.Gynecol Oncol. 2009 Sep;114(3):410-4. doi: 10.1016/j.ygyno.2009.04.037. Epub 2009 Jun 10. Gynecol Oncol. 2009. PMID: 19520420 Clinical Trial.
-
[Pegylated liposomal doxorubicin in ovarian cancer treatment].Ginekol Pol. 2009 Aug;80(8):615-9. Ginekol Pol. 2009. PMID: 19824461 Review. Polish.
-
What Characterizes Long-term Survivors of Recurrent Ovarian Cancer? Case Report and Review of the Literature.Anticancer Res. 2016 Oct;36(10):5365-5371. doi: 10.21873/anticanres.11110. Anticancer Res. 2016. PMID: 27798900 Review.
Cited by
-
Lipid-based nanosystems: a pivotal solution in drug delivery.Nanomedicine (Lond). 2025 Jan;20(2):121-123. doi: 10.1080/17435889.2024.2426969. Epub 2024 Nov 14. Nanomedicine (Lond). 2025. PMID: 39539220 No abstract available.
References
-
- Arduino PG, Bagan J, el-Naggar AK, Carrozzo M. Urban legends series: oral leukoplakia. Oral Dis 2013;19:642–59. - PubMed
-
- Scheifele C, Reichart PA. Is there a natural limit of the transformation rate of oral leukoplakia? Oral Oncol 2003;39:470–5. - PubMed
-
- Grady D, Greene J, Daniels TE, Ernster VL, Robertson PB, Hauck W et al. Oral mucosal lesions found in smokeless tobacco users. J Am Dent Assoc 1990;121:117–23. - PubMed
-
- Fonseca-Silva T, Diniz MG, de Sousa SF, Gomez RS, Gomes CC. Association between histopathological features of dysplasia in oral leukoplakia and loss of heterozygosity. Histopathology 2016;68:456–60. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
