

The Association of N-Terminal Pro-Brain Natriuretic Peptide With Time to Clinical Worsening in Hispanic Patients With Pulmonary Arterial Hypertension
- PMID: 35465086
- PMCID: PMC8993436
- DOI: 10.14740/cr1362
The Association of N-Terminal Pro-Brain Natriuretic Peptide With Time to Clinical Worsening in Hispanic Patients With Pulmonary Arterial Hypertension
Abstract
Background: Measurement of N-terminal pro-brain natriuretic peptide (NT-proBNP) level is an important parameter in the risk assessment of patients with pulmonary arterial hypertension (PAH). Data about the prognostic value of NT-proBNP in the Hispanic PAH population are lacking. Historically, clinical trials in PAH have only included a minority of Hispanic patients. It has been reported that baseline NT-proBNP levels differ between different ethnicities. Furthermore, NT-proBNP levels can be impacted by declining renal function, making its interpretation difficult regarding clinical decision making.
Methods: In a retrospective single-center cohort analysis, Hispanic patients with PAH had a baseline outpatient NT-proBNP level drawn during a period of clinical stability and were followed for 1 year to monitor for time to clinical worsening (TTCW). The association of baseline NT-proBNP and TTCW was assessed in patients with normal and abnormal renal function.
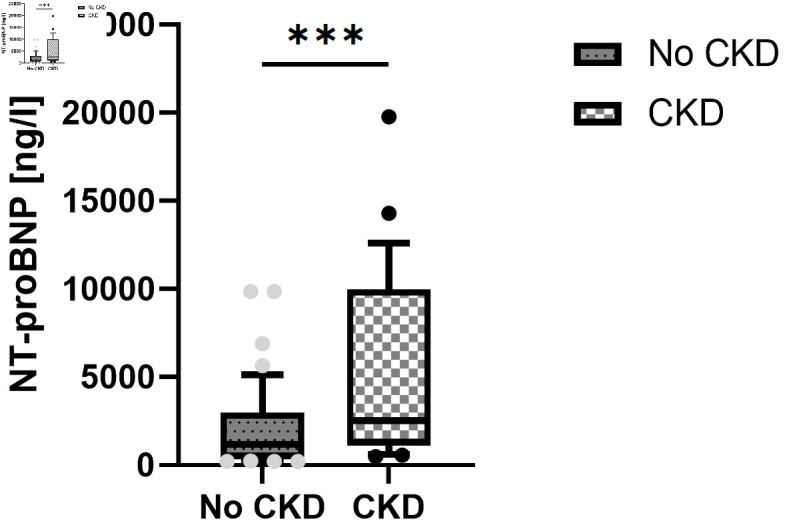
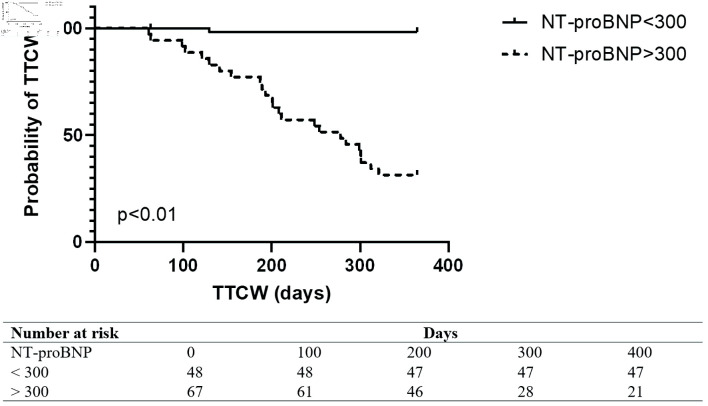
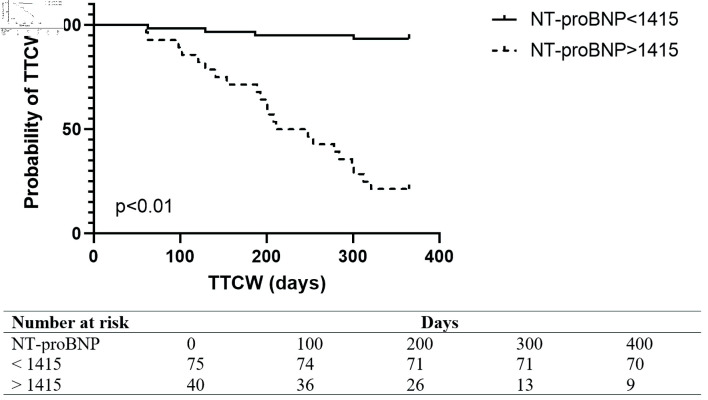
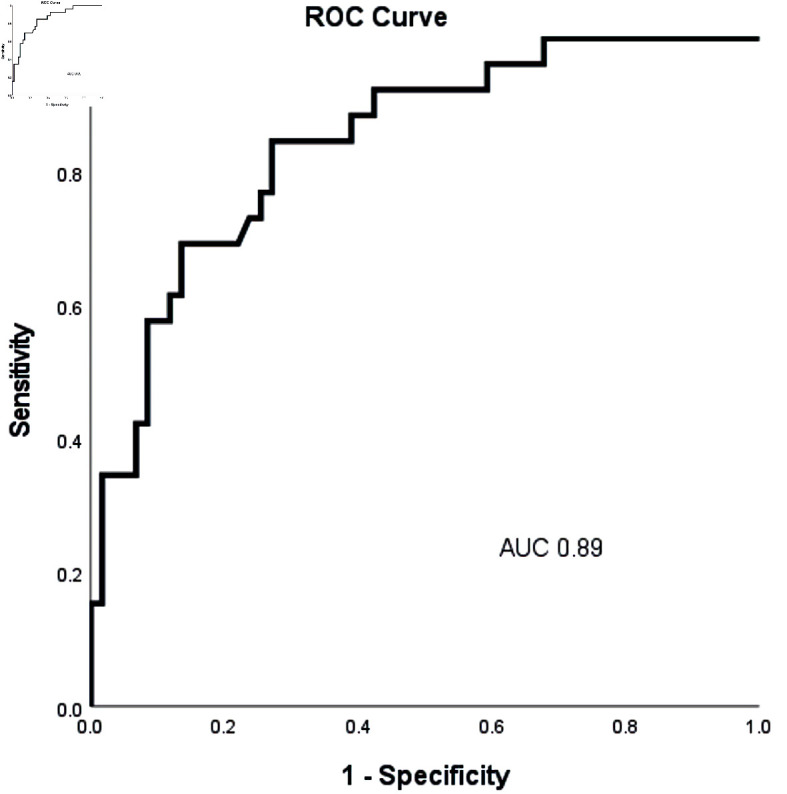
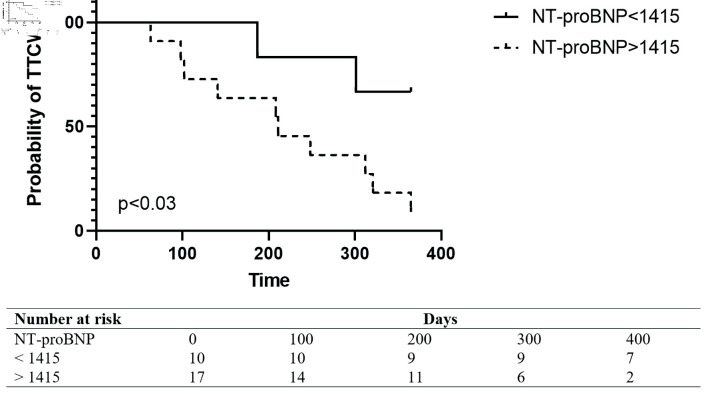
Results: A total of 26 patients (22%) met the clinical endpoint of clinical worsening. Twenty-seven patients (24%) had chronic kidney disease (CKD). At baseline NT-proBNP levels showed a significant inverse correlation with 6-min walk test (6MWD, r = -0.382, P = 0.02), and a significant positive correlation with renal function (r = 0.273, P = 0.05). NT-proBNP levels did not correlate with age (r = 0.19, P = 0.11) or body mass index (BMI) (r = -0.292, P = 0.061). NT-proBNP levels of > 1,415 ng/L were significantly associated with shorter TTCW (P < 0.01) in all patients and in patients with CKD (P = 0.03). A stepwise increase in NT-proBNP levels by 100 ng/L was associated with a higher risk of meeting the clinical endpoint of TTCW in patients with normal renal function (hazard ratio (HR) = 1.8, P < 0.01) and CKD (HR = 1.5, P < 0.01).
Conclusions: In Hispanic patients with PAH, NT-proBNP is a valuable tool to predict 1-year TTCW, independent of renal function.
Keywords: Hispanics; N-terminal pro-brain natriuretic peptide; Pulmonary arterial hypertension.
Copyright 2022, Khatab et al.
Conflict of interest statement
There is no potential conflict of interest to be declared by the authors.
Figures
References
-
- Chin KM, Rubin LJ, Channick R, Di Scala L, Gaine S, Galie N, Ghofrani HA. et al. Association of N-terminal pro brain natriuretic peptide and long-term outcome in patients with pulmonary arterial hypertension. Circulation. 2019;139(21):2440–2450. doi: 10.1161/CIRCULATIONAHA.118.039360. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous