

Outcomes of Endurant II Stent Graft According to Anatomic Severity Grade Score
- PMID: 35466775
- PMCID: PMC10868145
- DOI: 10.1177/15266028221090433
Outcomes of Endurant II Stent Graft According to Anatomic Severity Grade Score
Abstract
Objectives: This study's objective was to evaluate Endurant II (Medtronic Inc, Minneapolis, Minnesota) stent graft's early and midterm outcomes and compare the results according to the anatomic severity grade (ASG) scores.
Methods: This was a retrospective study of patients treated with the Endurant II stent graft between January 2013 and May 2021. The patients were divided into 2 independent groups, including those with a low ASG score (score <14) and a high ASG score (score >14).
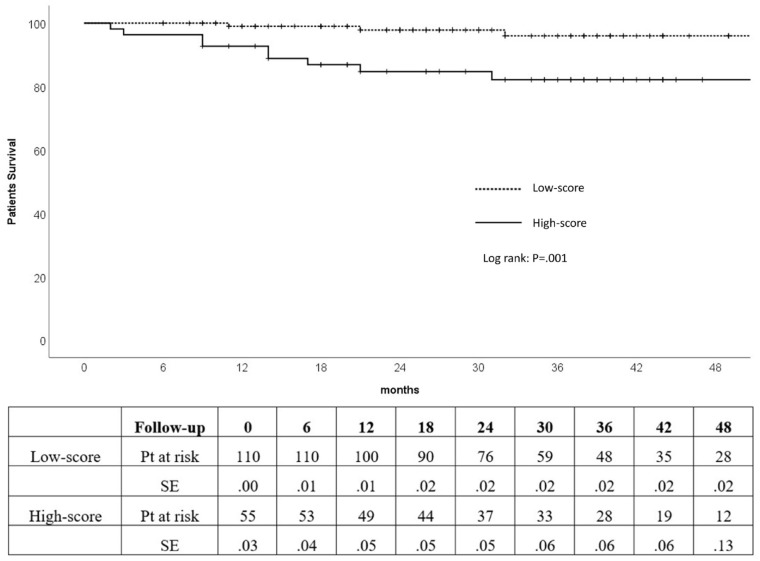
Results: A total of 165 consecutive patients (89% males, age 74±8 years) were included. There were 110 (67%) patients in the low-score group and 55 (33%) patients in the high-score group. Technical success was achieved in all cases. Primary clinical success at 30 days was 100% and at 1 year was 96%. Median operative time was longer in the high-score group with no statistical significance (133 vs 120 minutes, p=0.116). The median dose area product of low-score patients (50.9 Gy·cm2; IQR 22.4-75.5 Gy·cm2) was significantly lower than high-score patients (85.0 Gy·cm2; IQR 46.5-127.9 Gy·cm2) with p=0.025. Median fluoroscopic time was lower in low-score patients (17 minutes; IQR 13-24 minutes) compared with high-score patients (19 minutes; IQR 16-23 minutes) without a significant difference at p=0.148. At a midterm follow-up of 32 months (range 2-63 months), combined complications (29% vs 8%, p<0.001) and implant-related complications (13% vs 4%, p=0.043) were higher in the high-score group. Systemic complications at 30 days were higher in the high-score group without a statistically significant difference (15% vs 11%, p=0.500). The Kaplan-Meier estimate of freedom from reintervention was significantly higher in the low-risk group at 1 (97% vs 90%), 2 (96% vs 88%), and 3 years (96% vs 85%) with (p=0.035). The cumulative survival rate was significantly higher in the low-score group than high-score group (p=0.001) at 1 (99% vs 87%), 2 (98% vs 85%), and 3 years (96% vs 82%).
Conclusions: Endurant II endovascular aneurysm repair seems to be safe in both low-score and high-score patients. However, patients in the high-score group showed more implant-related complications and midterm mortalities than those in the low-score group.
Keywords: ASG score; EVAR; Endurant II; abdominal aortic aneurysm; stent graft.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures


References
MeSH terms
LinkOut - more resources
Full Text Sources
