

Complex adult congenital heart disease on cross-sectional imaging: an introductory overview
- PMID: 35467233
- PMCID: PMC9038985
- DOI: 10.1186/s13244-022-01201-y
Complex adult congenital heart disease on cross-sectional imaging: an introductory overview
Abstract
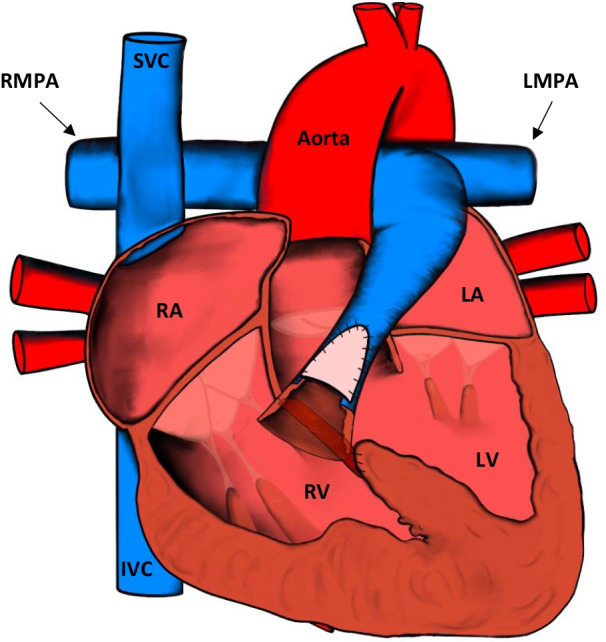
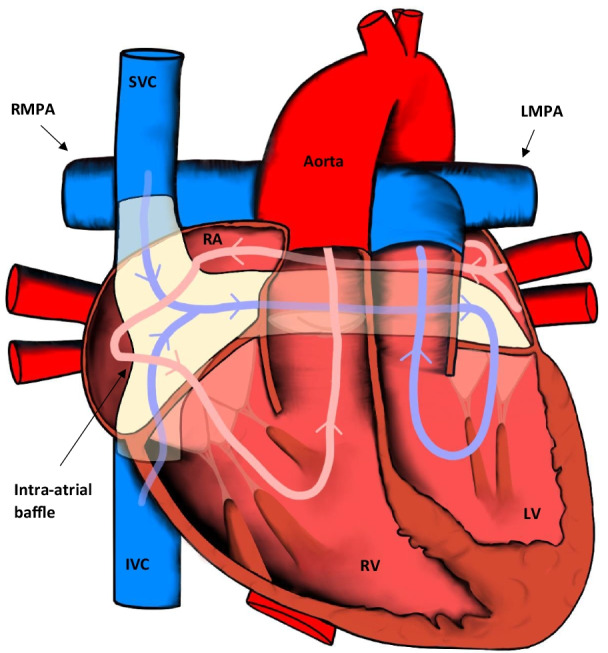
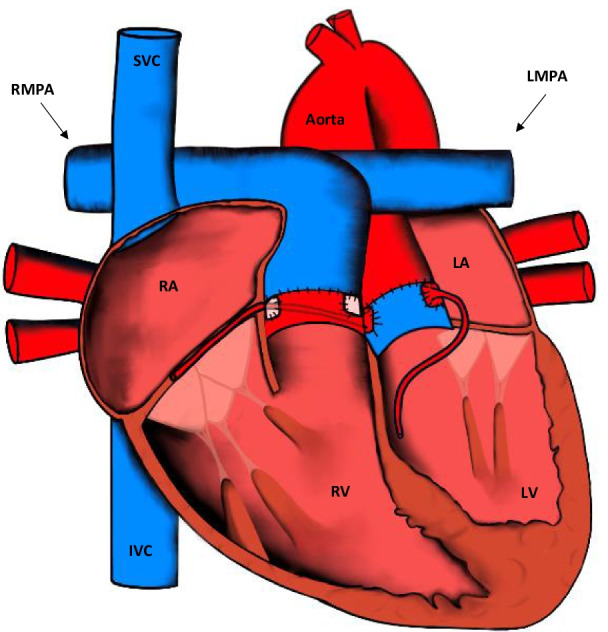
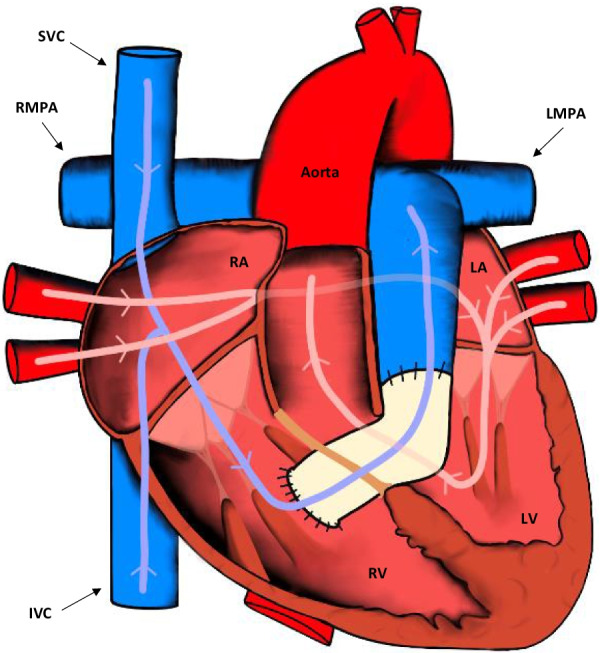
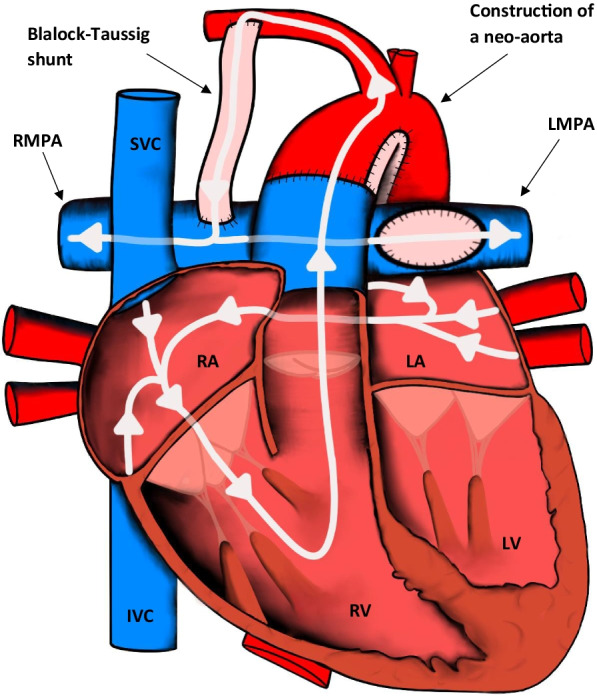
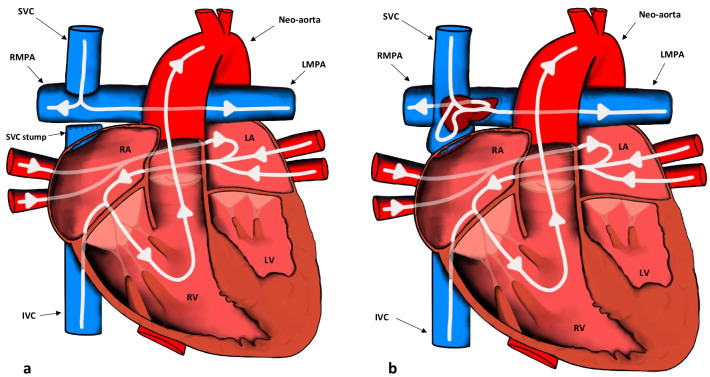
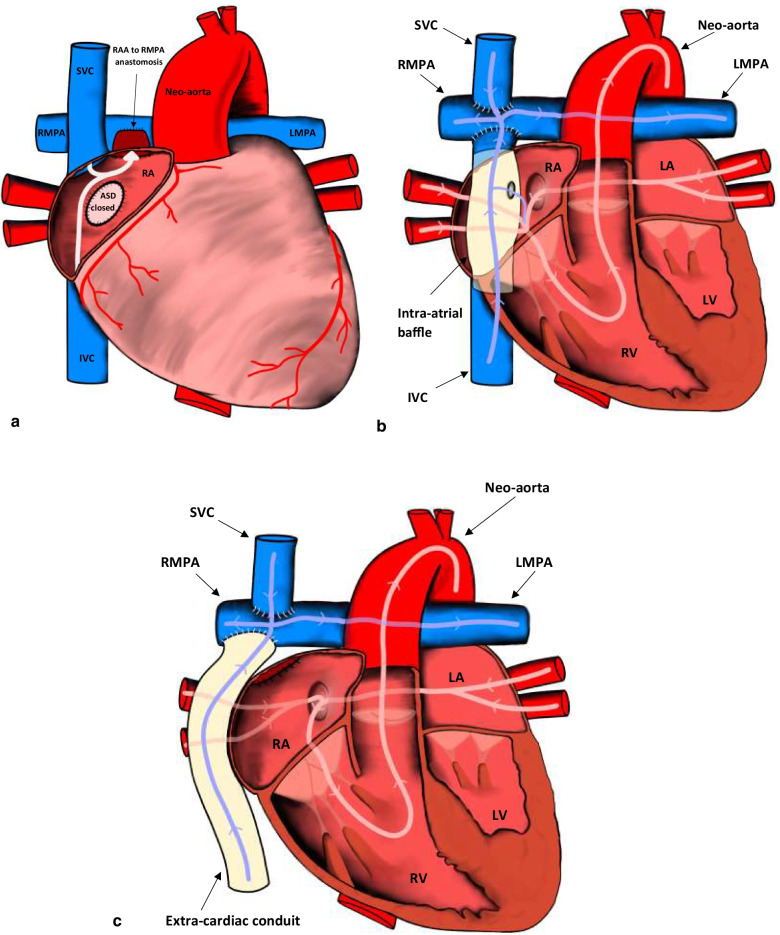
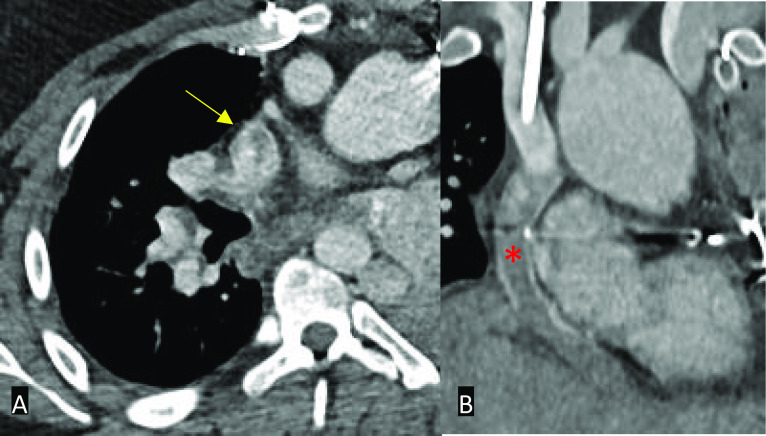
Congenital heart disease is the most common group of congenital pathology. Over the past few decades, advances in surgical treatment have resulted in a rising population of adult patients with repaired complex congenital heart disease. Although the quality of life has greatly improved, a significant proportion of morbidities encountered in clinical practice is now seen in adults rather than in children. These patients often have significant haemodynamic pathophysiology necessitating repeat intervention. CT and MRI are excellent imaging modalities, which help elucidate potential complications that may need urgent management. Although imaging should be performed in specialised centres, occasionally patients may present acutely to emergency departments in hospitals with little experience in managing potentially complex patients. The purpose of this article is to provide an introductory overview to the radiologist who may not be familiar with complex congenital heart disease in adult patients. This educational review has three main sections: (1) a brief overview of the post-operative anatomy and surgical management of the most common complex conditions followed by (2) a discussion on CT/MRI protocols and (3) a review of the various complications and their CT/MRI findings.
Keywords: Adult congenital heart disease; Computed tomography (CT); Magnetic resonance imaging (MRI).
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Stout KK, Daniels CJ, Aboulhosn JA, et al. 2018 AHA/ACC guideline for the management of adults with congenital heart disease: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. Circulation. 2019;139:e698–e800. - PubMed
-
- Sachdeva R, Valente AM, Armstrong AK, et al. ACC/AHA/ASE/HRS/ISACHD/SCAI/SCCT/SCMR/SOPE 2020 appropriate use criteria for multimodality imaging during the follow up care of patients with congenital heart disease: a report of the American College of Cardiology solution set oversight committee and appropriate use criteria task force, American Heart Association, American Society of Echocardiography, Heart Rhythm Society, International Society for Adult Congenital Heart Disease, Society for Cardiovascular Angiography and Interventions, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance, and Society of Pediatric Echocardiography. J Am Coll Cardiol. 2020;75:657–703. doi: 10.1016/j.jacc.2019.10.002. - DOI - PubMed
-
- Araujo JJ. The profile of an adult with congenital heart disease. Int J Clin Cardiol. 2018;5:131.
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
