

Radiology-pathology correlation of endometrial carcinoma assessment on magnetic resonance imaging
- PMID: 35467253
- PMCID: PMC9038982
- DOI: 10.1186/s13244-022-01218-3
Radiology-pathology correlation of endometrial carcinoma assessment on magnetic resonance imaging
Abstract
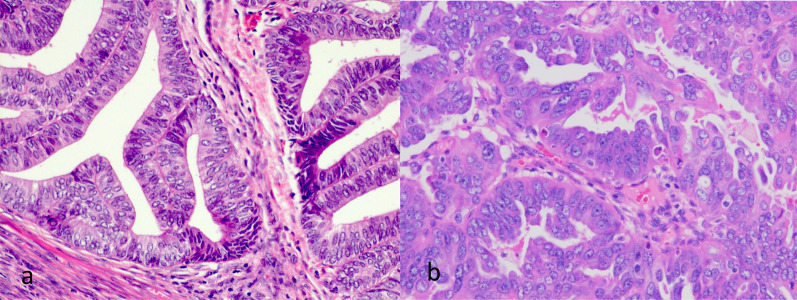
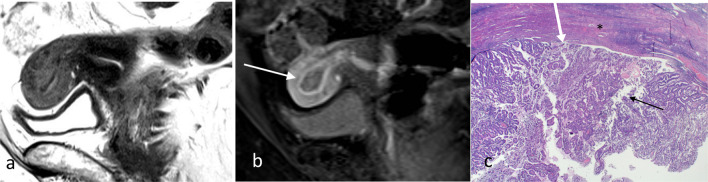
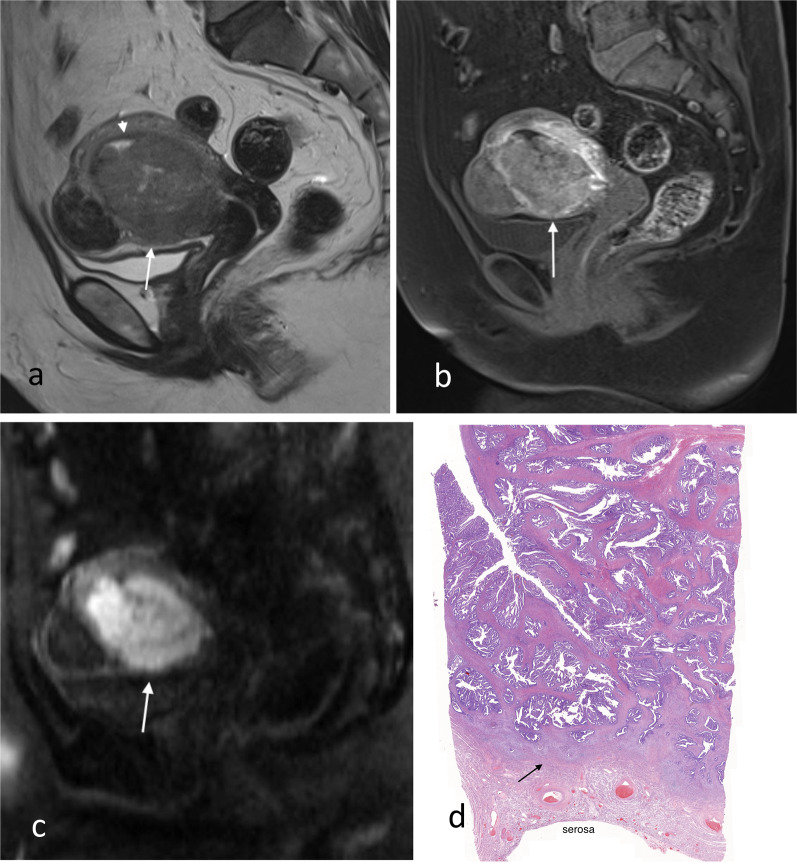
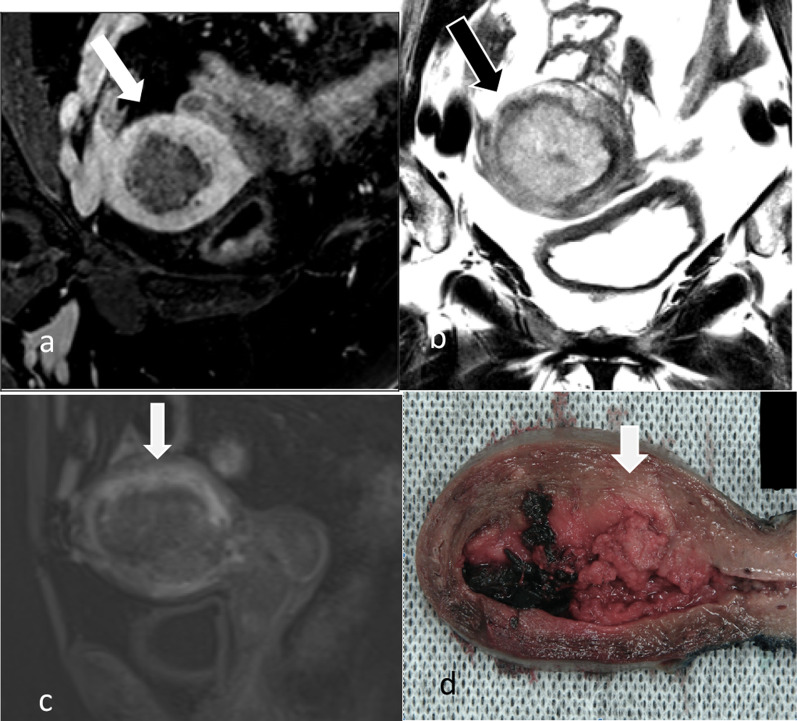
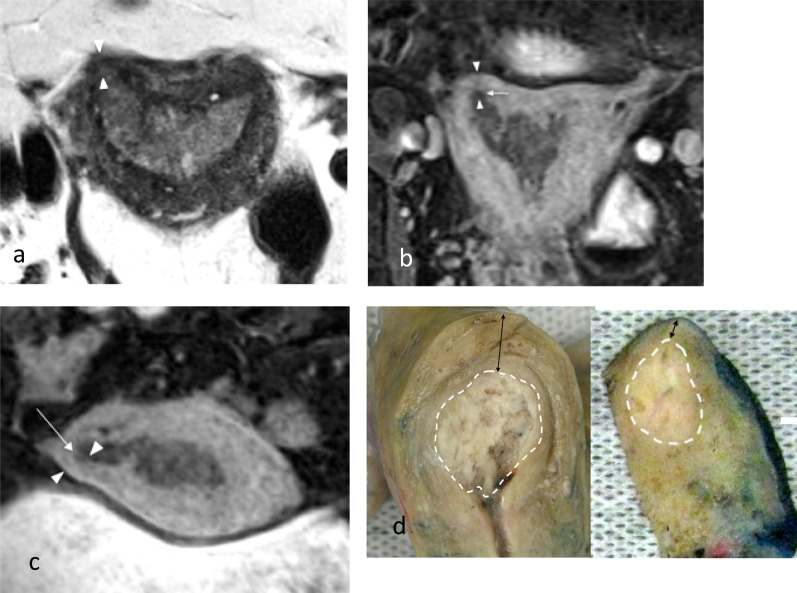
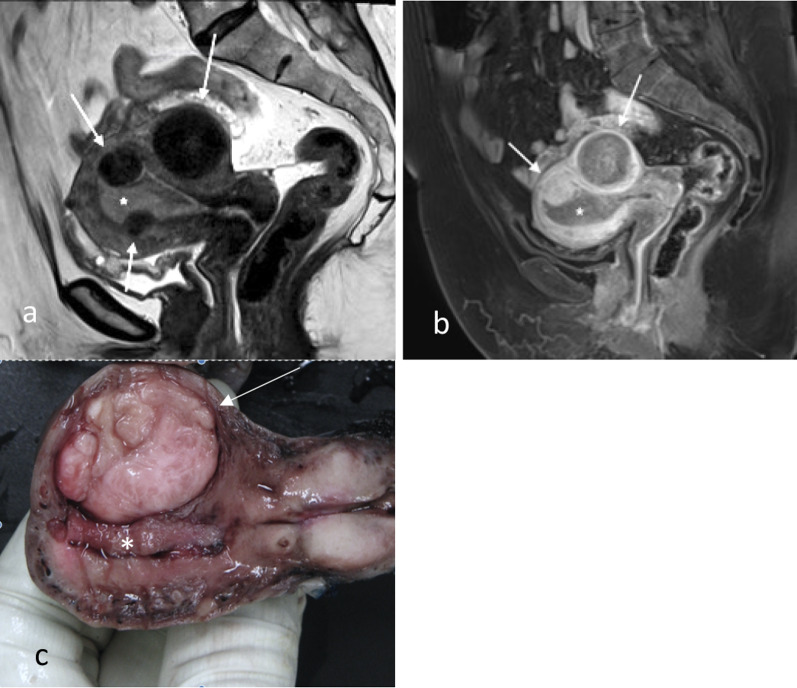
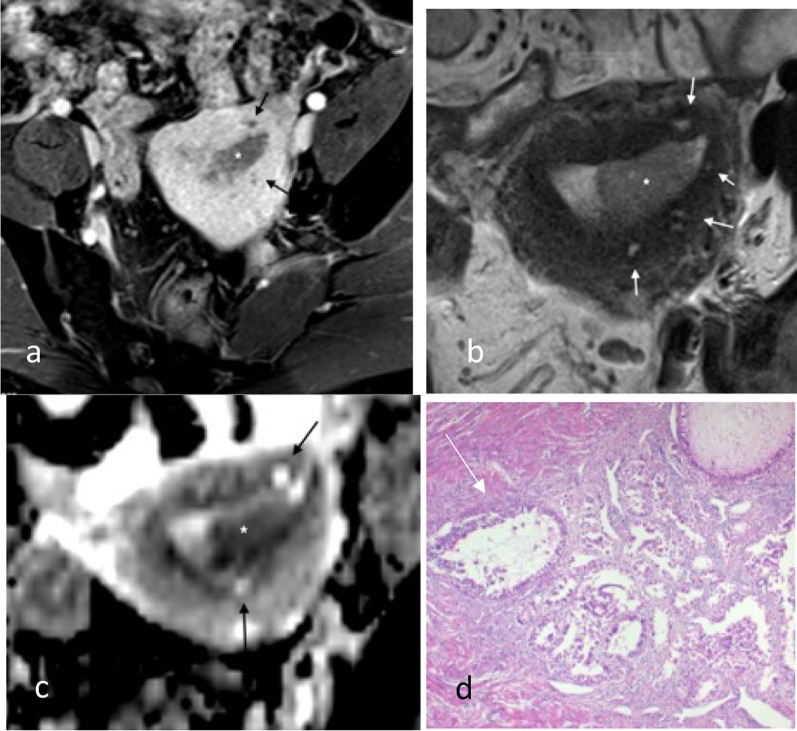
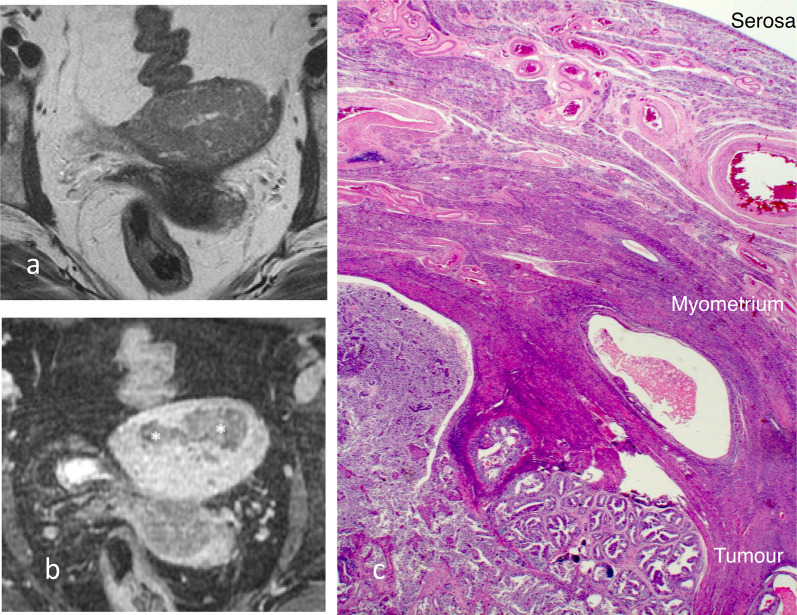
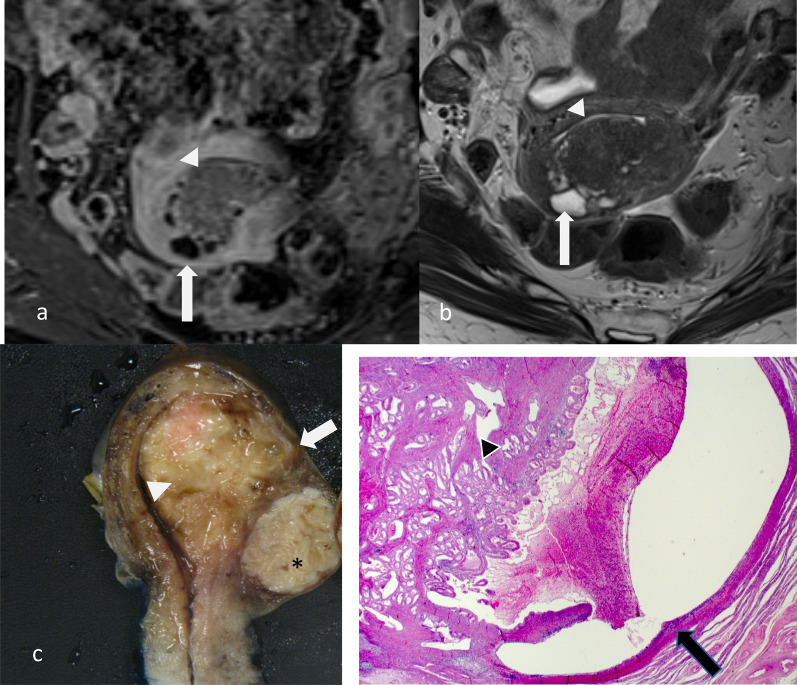
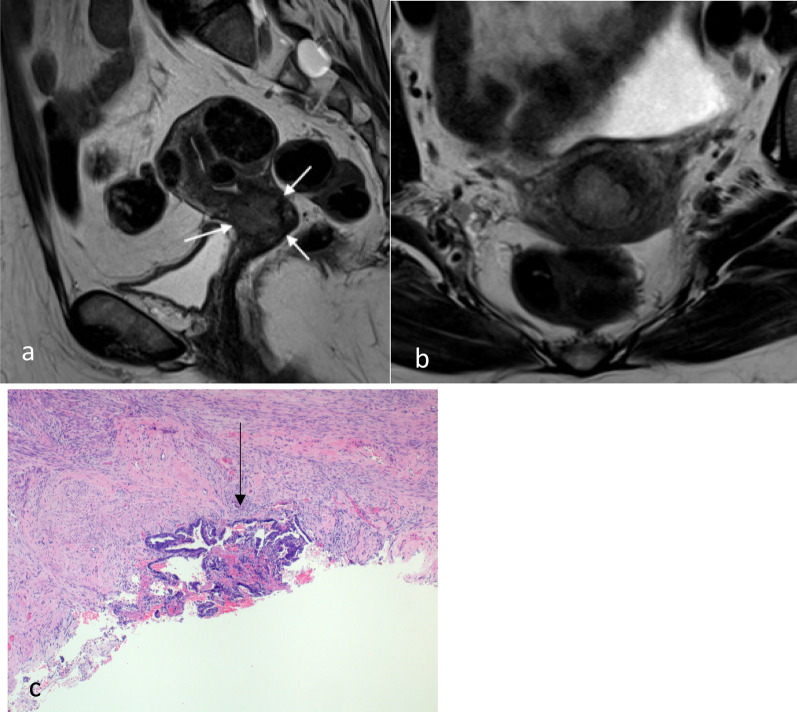
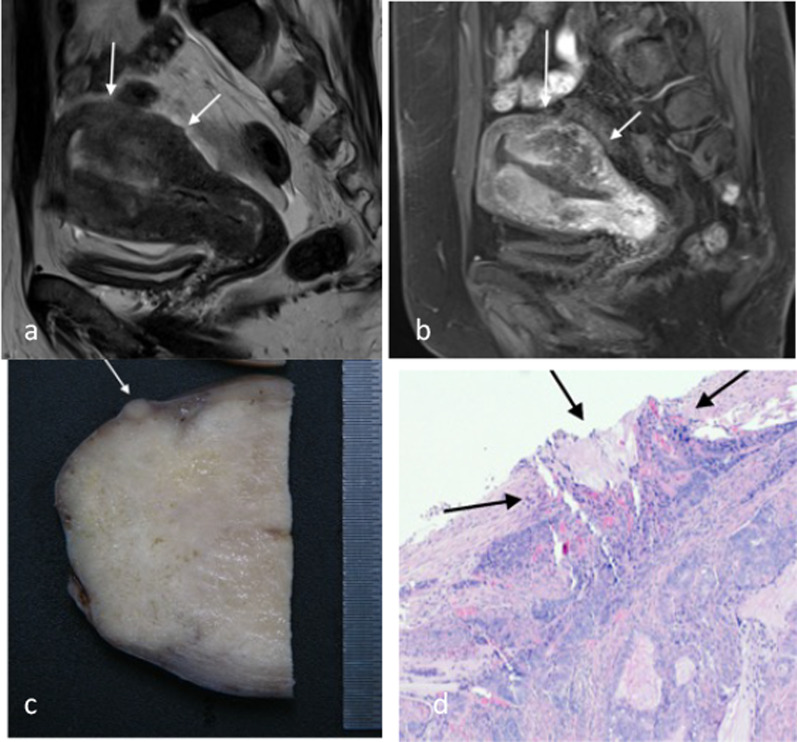
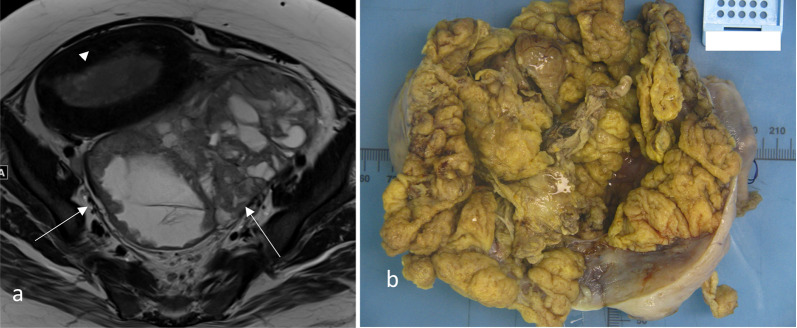
Endometrial carcinoma is the most common gynaecological cancer in developed countries. Most cases are low-volume/low-grade tumour at presentation; however, high-grade subtypes may present with locally advanced disease with higher propensity for spread outside of the pelvis. MRI has a role in local staging of the tumour and helping the clinicians in treatment decision making. This pictorial essay gives examples of endometrial carcinoma at different stages with histological correlation. It also explores the potential limitations and pitfalls of imaging in this context.
Keywords: Endometrial carcinoma; FIGO staging; Magnetic resonance imaging; Radiology-pathology correlation.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Brand A, Hammond I, Cheuk R et al (2020) Clinical practice guidelines for the treatment and management of endometrial cancer. Cancer Council
-
- Otero-Garcia MM, Mesa-Alvarez A, Nikolic O, Blanco-Lobato P, Basta-Nikolic M, de Llano-Ortega RM, Paredes-Velazquez L, Nikolic N, Szewczyk-Bieda M. Role of MRI in staging and follow-up of endometrial and cervical cancer: pitfalls and mimickers. Insights Imaging. 2019;10(1):19. doi: 10.1186/s13244-019-0696-8. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
