

Prospective validation of a transcriptomic severity classifier among patients with suspected acute infection and sepsis in the emergency department
- PMID: 35467566
- PMCID: PMC9432813
- DOI: 10.1097/MEJ.0000000000000931
Prospective validation of a transcriptomic severity classifier among patients with suspected acute infection and sepsis in the emergency department
Abstract
Background and importance: mRNA-based host response signatures have been reported to improve sepsis diagnostics. Meanwhile, prognostic markers for the rapid and accurate prediction of severity in patients with suspected acute infections and sepsis remain an unmet need. IMX-SEV-2 is a 29-host-mRNA classifier designed to predict disease severity in patients with acute infection or sepsis.
Objective: Validation of the host-mRNA infection severity classifier IMX-SEV-2.
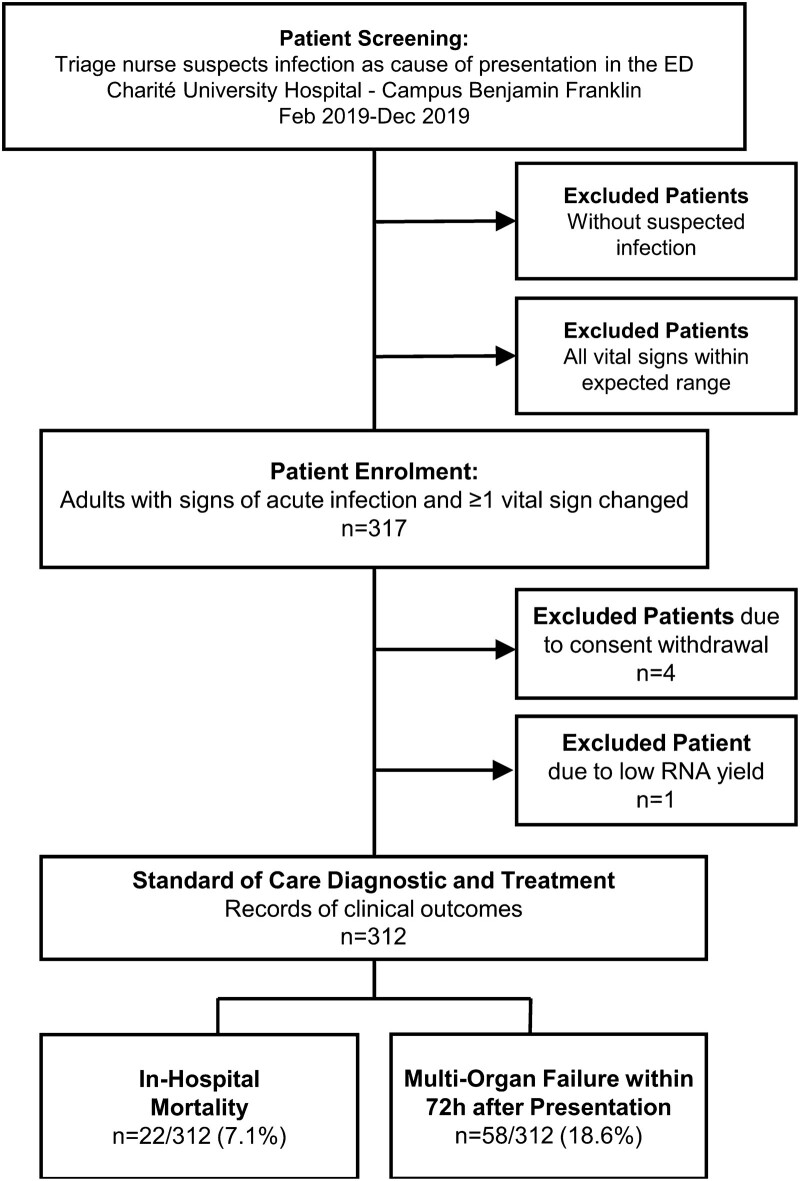
Design, settings and participants: Prospective, observational, convenience cohort of emergency department (ED) patients with suspected acute infections.
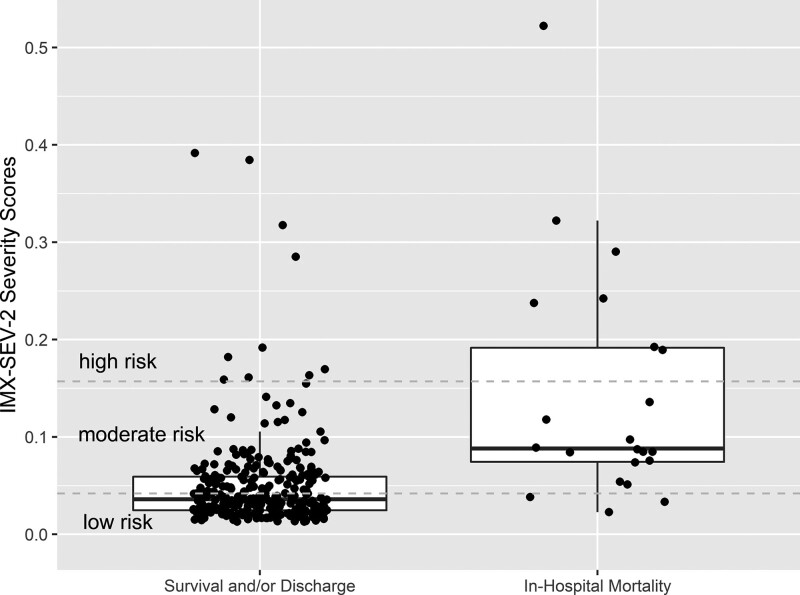
Outcome measures and analysis: Whole blood RNA tubes were analyzed using independently trained and validated composite target genes (IMX-SEV-2). IMX-SEV-2-generated risk scores for severity were compared to the patient outcomes in-hospital mortality and 72-h multiorgan failure.
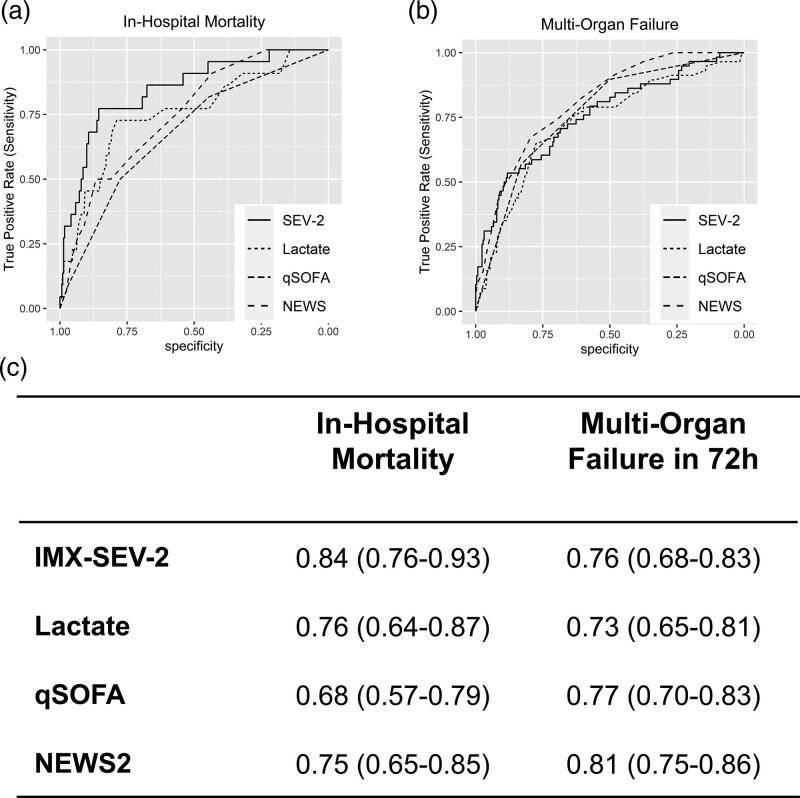
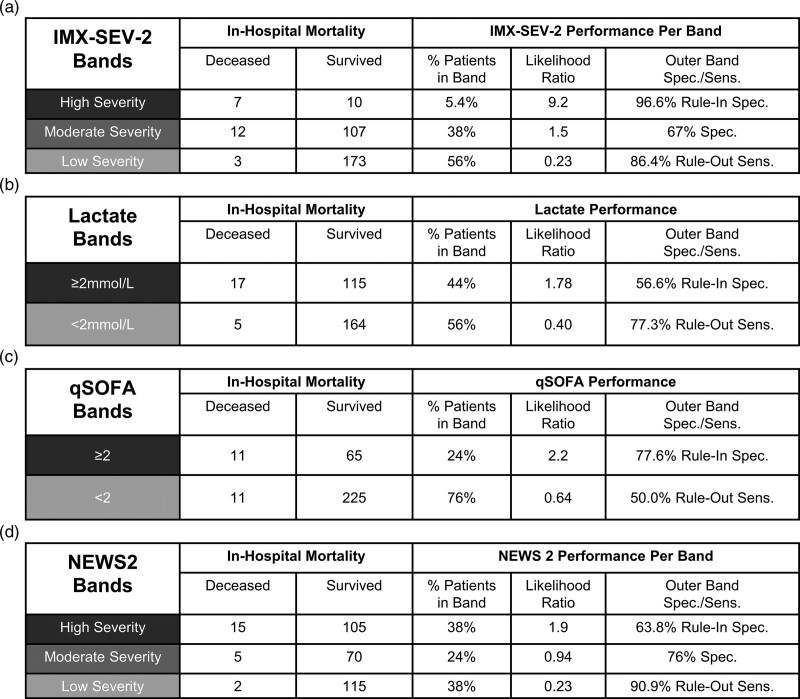
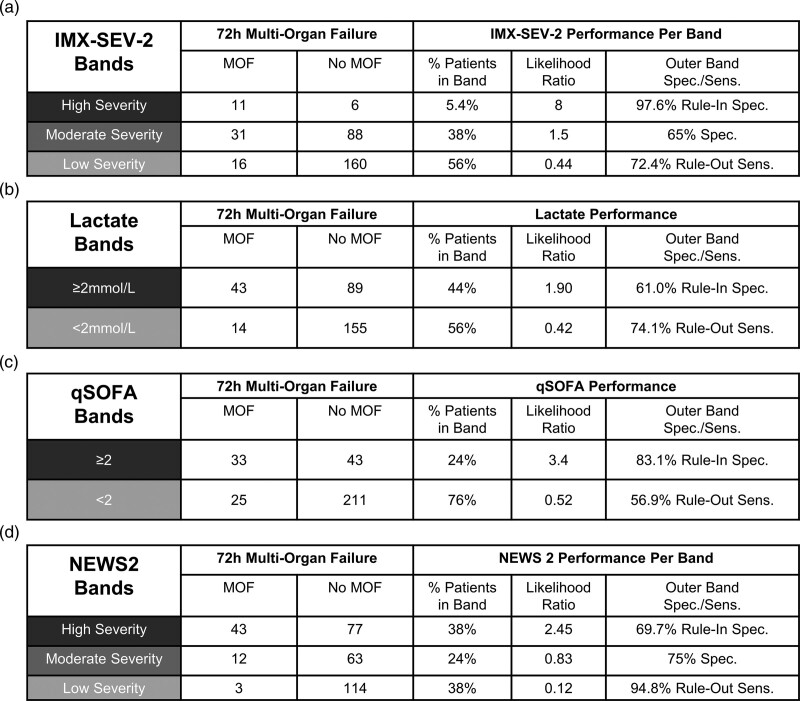
Main results: Of the 312 eligible patients, 22 (7.1%) died in hospital and 58 (18.6%) experienced multiorgan failure within 72 h of presentation. For predicting in-hospital mortality, IMX-SEV-2 had a significantly higher area under the receiver operating characteristic (AUROC) of 0.84 [95% confidence intervals (CI), 0.76-0.93] compared to 0.76 (0.64-0.87) for lactate, 0.68 (0.57-0.79) for quick Sequential Organ Failure Assessment (qSOFA) and 0.75 (0.65-0.85) for National Early Warning Score 2 (NEWS2), ( P = 0.015, 0.001 and 0.013, respectively). For identifying and predicting 72-h multiorgan failure, the AUROC of IMX-SEV-2 was 0.76 (0.68-0.83), not significantly different from lactate (0.73, 0.65-0.81), qSOFA (0.77, 0.70-0.83) or NEWS2 (0.81, 0.75-0.86).
Conclusion: The IMX-SEV-2 classifier showed a superior prediction of in-hospital mortality compared to biomarkers and clinical scores among ED patients with suspected infections. No improvement for predicting multiorgan failure was found compared to established scores or biomarkers. Identifying patients with a high risk of mortality or multiorgan failure may improve patient outcomes, resource utilization and guide therapy decision-making.
Copyright © 2022 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The institution of N.G., E.D.W., D.L., N.M., W.H.B., R.T., K.K., R.S. and W.B received funding from Inflammatix. J.W., O.L., M.M., L.B., R.L. and T.E.S are employees of and option shareholders in Inflammatix. N.G. received a travel grant from Inflammatix, Inc. to attend a conference.
Figures
References
-
- Kaukonen KM, Bailey M, Pilcher D, Cooper DJ, Bellomo R. Systemic inflammatory response syndrome criteria in defining severe sepsis. N Engl J Med 2015; 372:1629–1638. - PubMed
-
- Yealy DM, Mohr NM, Shapiro NI, Venkatesh A, Jones AE, Self WH. Early care of adults with suspected sepsis in the emergency department and out-of-hospital environment: a consensus-based task force report. Ann Emerg Med 2021; 78:1–19. - PubMed
-
- McCreery RJ, Florescu DF, Kalil AC. Sepsis in immunocompromised patients without human immunodeficiency virus. J Infect Dis 2020; 222:S156–S165. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
