

Evaluation of a Slipped Capital Femoral Epiphysis Virtual Reality Surgical Simulation for the Orthopaedic Trainee
- PMID: 35467580
- PMCID: PMC9042586
- DOI: 10.5435/JAAOSGlobal-D-22-00028
Evaluation of a Slipped Capital Femoral Epiphysis Virtual Reality Surgical Simulation for the Orthopaedic Trainee
Abstract
Objective: The purpose of this study was to compare outcomes between orthopaedic trainees using various preoperative training platforms (physical simulation [PS], virtual reality [VR], and reading/videos) in a slipped capital femoral epiphysis model.
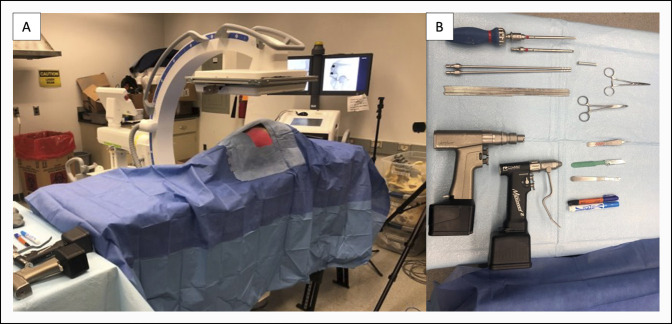
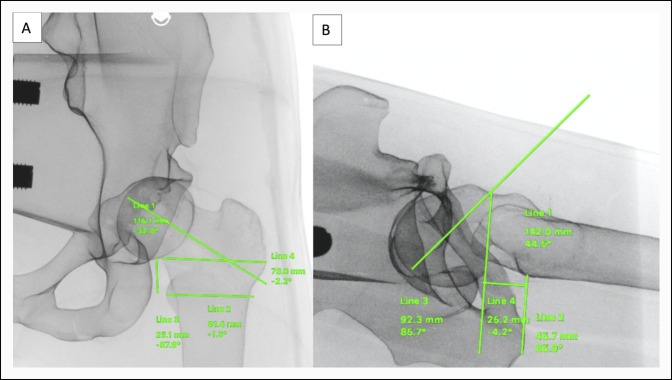
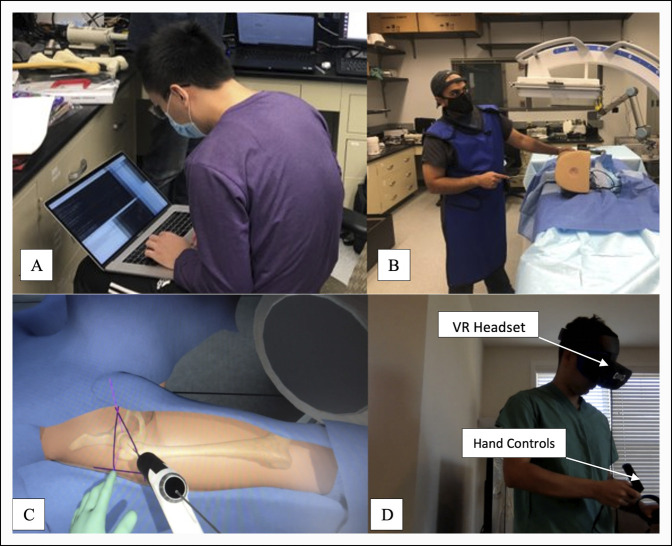
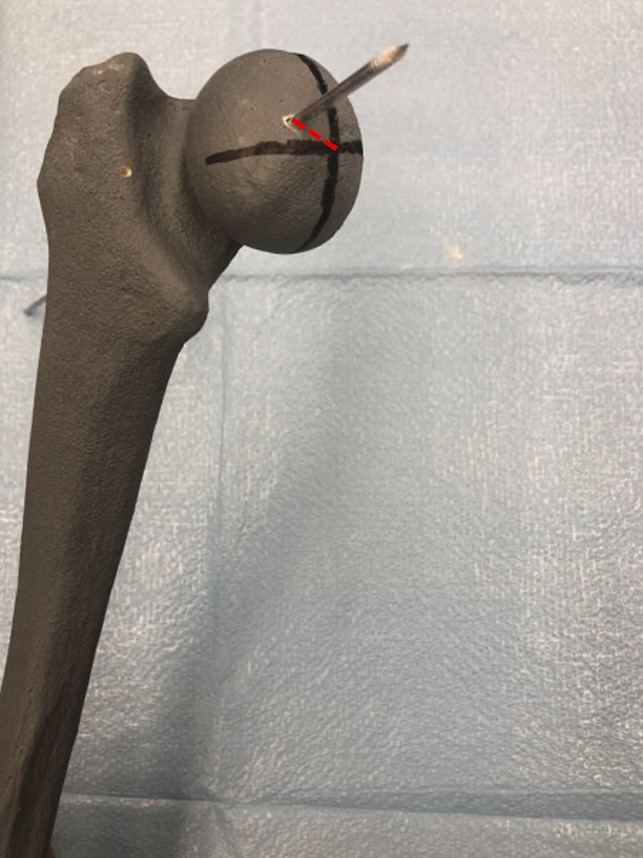
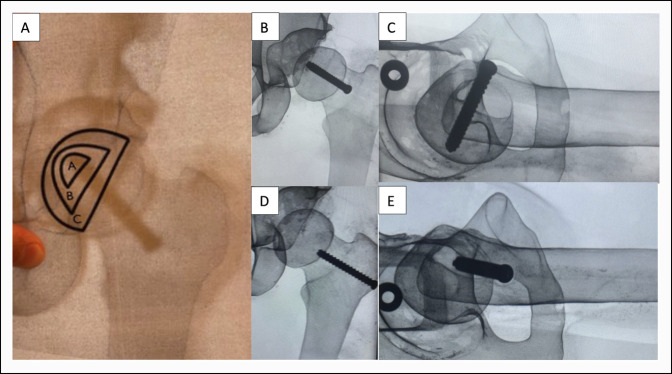
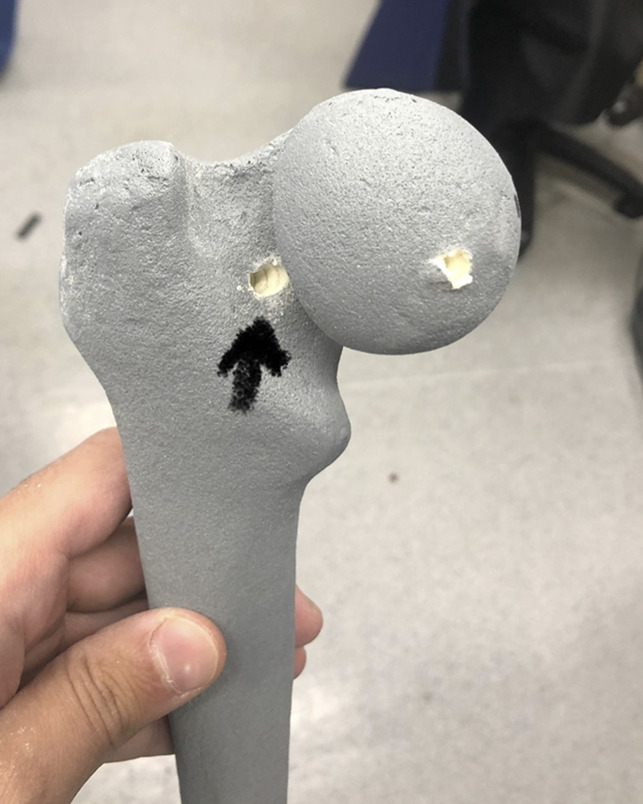
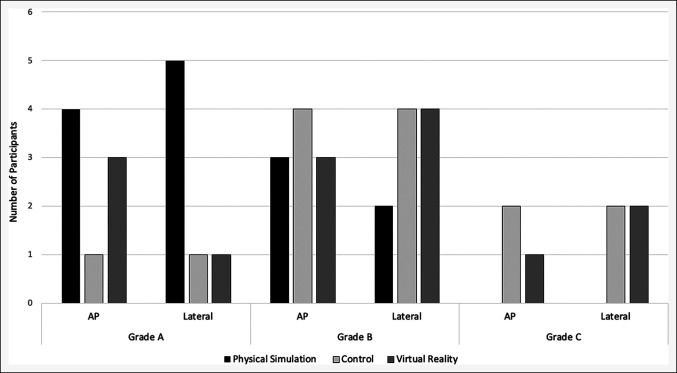
Methods: Participants were randomly assigned to one of the three groups: (1) reading/video control group (n = 7), (2) VR group (n = 7), or (3) PS group (n = 7). Participants in the VR group completed a VR slipped capital femoral epiphysis module while participants in the PS group practiced the placement of a screw in the physical module before evaluation of percutaneous screw placement in the PS model. Outcomes evaluated included overall surgical time, amount of fluoroscopy, Global Rating Scale score, radiographic screw position, physical screw accuracy, presence of breeching of the articular surface or femoral neck, and overall platform rating (0 to 10).
Results: No difference was observed in surgical time, Global Rating Scale score, radiographic or physical accuracy of screw position, or articular surface breaching between the groups. Subjectively, there was a difference in utility of platform rating between the groups (PS: 10 ± 0, VR: 7 ± 2, and control: 6 ± 1, P = 0.001).
Conclusion: Training with VR was subjectively rated higher in value compared with reading/video methods and had similar performance outcomes compared with training with PS.
Copyright © 2022 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Orthopaedic Surgeons.
Figures

Similar articles
-
The Utility of Virtual Reality in Orthopedic Surgical Training.J Surg Educ. 2022 Nov-Dec;79(6):1516-1525. doi: 10.1016/j.jsurg.2022.06.007. Epub 2022 Jul 9. J Surg Educ. 2022. PMID: 35821110 Free PMC article. Clinical Trial.
-
Oblique in situ screw fixation of stable slipped capital femoral epiphysis.J Pediatr Orthop. 2013 Mar;33(2):135-8. doi: 10.1097/BPO.0b013e318277d02d. J Pediatr Orthop. 2013. PMID: 23389566
-
Arthrogram-assisted fixation of slipped capital femoral epiphysis: a CT and radiographic study.J Pediatr Orthop. 2012 Oct-Nov;32(7):693-6. doi: 10.1097/BPO.0b013e31826bb1d0. J Pediatr Orthop. 2012. PMID: 22955533
-
Mechanical failure of single cannulated screw fixation of unstable slipped capital femoral epiphysis.J Pediatr Orthop B. 2014 Jan;23(1):49-54. doi: 10.1097/BPB.0b013e328364eb74. J Pediatr Orthop B. 2014. PMID: 23912908 Review.
-
Slipped Capital Femoral Epiphysis: The European Perspective.J Pediatr Orthop. 2018 Jul;38 Suppl 1:S1-S4. doi: 10.1097/BPO.0000000000001161. J Pediatr Orthop. 2018. PMID: 29877936 Review.
Cited by
-
Virtual Reality and Surgical Simulation Training for Orthopaedic Surgery Residents: A Qualitative Assessment of Trainee Perspectives.JB JS Open Access. 2024 Mar 20;9(1):e23.00142. doi: 10.2106/JBJS.OA.23.00142. eCollection 2024 Jan-Mar. JB JS Open Access. 2024. PMID: 38511201 Free PMC article. Review.
-
Extended reality for biomedicine.Nat Rev Methods Primers. 2023;3:15. doi: 10.1038/s43586-023-00208-z. Epub 2023 Mar 2. Nat Rev Methods Primers. 2023. PMID: 37051227 Free PMC article.
-
Application of Virtual Reality Systems in Bone Trauma Procedures.Medicina (Kaunas). 2023 Mar 14;59(3):562. doi: 10.3390/medicina59030562. Medicina (Kaunas). 2023. PMID: 36984563 Free PMC article. Review.
References
-
- Banaszek D, You D, Chang J, et al. : Virtual reality compared with bench-top simulation in the acquisition of arthroscopic skill: A randomized controlled trial. J Bone Joint Surg Am 2017;99:e34. - PubMed
-
- Camp CL, Krych AJ, Stuart MJ, Regnier TD, Mills KM, Turner NS: Improving resident performance in knee arthroscopy: A prospective value assessment of simulators and cadaveric skills laboratories. J Bone Joint Surg Am 2016;98:220-225. - PubMed
-
- Cannon WD, Garrett WE, Hunter RE, et al. : Improving residency training in arthroscopic knee surgery with use of a virtual-reality simulator: A randomized blinded study. J Bone Joint Surg Am 2014;96:1798-1806. - PubMed
-
- Logishetty K, Rudran B, Cobb JP: Virtual reality training improves trainee performance in total hip arthroplasty: A randomized controlled trial. Bone Joint J 2019;101-B:1585-1592. - PubMed
-
- Rebolledo BJ, Hammann-Scala J, Leali A, Ranawat AS: Arthroscopy skills development with a surgical simulator: A comparative study in orthopaedic surgery residents. Am J Sports Med 2015;43:1526-1529. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
