

SARS-CoV-2 seroprevalence among healthcare workers
- PMID: 35468153
- PMCID: PMC9037906
- DOI: 10.1371/journal.pone.0266410
SARS-CoV-2 seroprevalence among healthcare workers
Abstract
Background: Monitoring COVID-19 infection risk among health care workers (HCWs) is a public health priority. We examined the seroprevalence of SARS-CoV-2 among HCWs following the fall infection surge in Minnesota, and before and after COVID-19 vaccination. Additionally, we assessed demographic and occupational risk factors for SARS-CoV-2 infection.
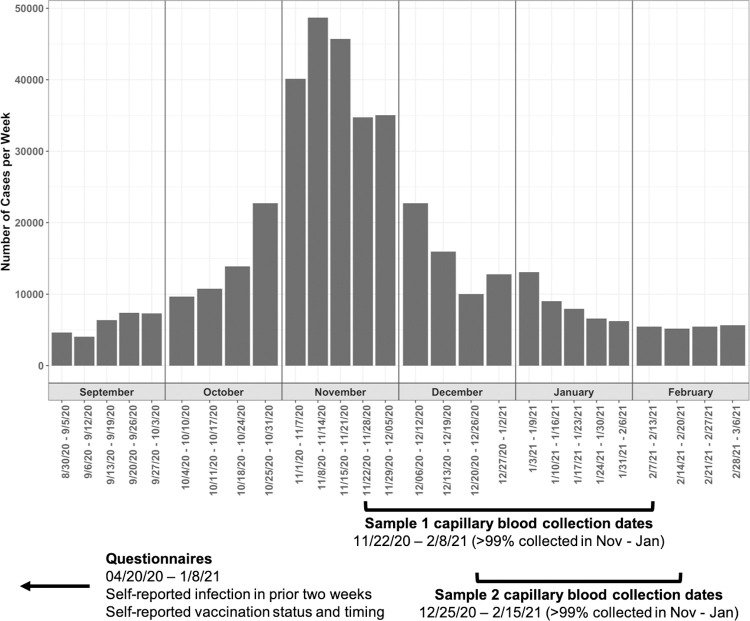
Methods: We conducted two rounds of seroprevalence testing among a cohort of HCWs: samples in round 1 were collected from 11/22/20-02/21/21 and in round 2 from 12/18/20-02/15/21. Demographic and occupational exposures assessed with logistic regression were age, sex, healthcare role and setting, and number of children in the household. The primary outcome was SARS-CoV-2 IgG seropositivity. A secondary outcome, SARS-CoV-2 infection, included both seropositivity and self-reported SARS-CoV-2 test positivity.
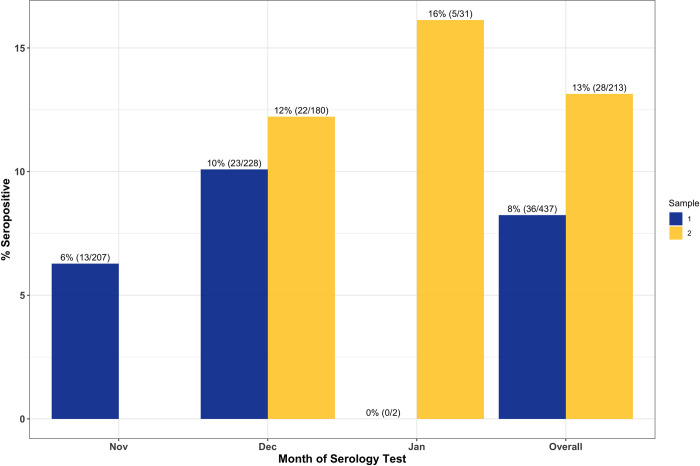
Results: In total, 459 HCWs were tested. 43/454 (9.47%) had a seropositive sample 1 and 75/423 (17.7%) had a seropositive sample 2. By time of sample 2 collection, 54% of participants had received at least one vaccine dose and seroprevalence was 13% among unvaccinated individuals. Relative to physicians, the odds of SARS-CoV-2 infection in other roles were increased (Nurse Practitioner: OR[95%CI] 1.93[0.57,6.53], Physician's Assistant: 1.69[0.38,7.52], Nurse: 2.33[0.94,5.78], Paramedic/EMTs: 3.86[0.78,19.0], other: 1.68[0.58,4.85]). The workplace setting was associated with SARS-CoV-2 infection (p = 0.04). SARS-CoV-2 seroprevalence among HCWs reporting duties in the ICU vs. those working in an ambulatory clinic was elevated: OR[95%CI] 2.17[1.01,4.68].
Conclusions: SARS-CoV-2 seroprevalence in HCW increased during our study period which was consistent with community infection rates. HCW role and setting-particularly working in the ICU-is associated with higher risk for SARS-CoV-2 infection.
Conflict of interest statement
Dr. Baumgartner is employed by Quansys Biosciences (Utah, USA), the manufacturer and testing site of the assays used. There are no patents, products in development, or marketed products associated with this research to declare. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures



References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
