

Systemic and mucosal IgA responses are variably induced in response to SARS-CoV-2 mRNA vaccination and are associated with protection against subsequent infection
- PMID: 35468942
- PMCID: PMC9037584
- DOI: 10.1038/s41385-022-00511-0
Systemic and mucosal IgA responses are variably induced in response to SARS-CoV-2 mRNA vaccination and are associated with protection against subsequent infection
Abstract
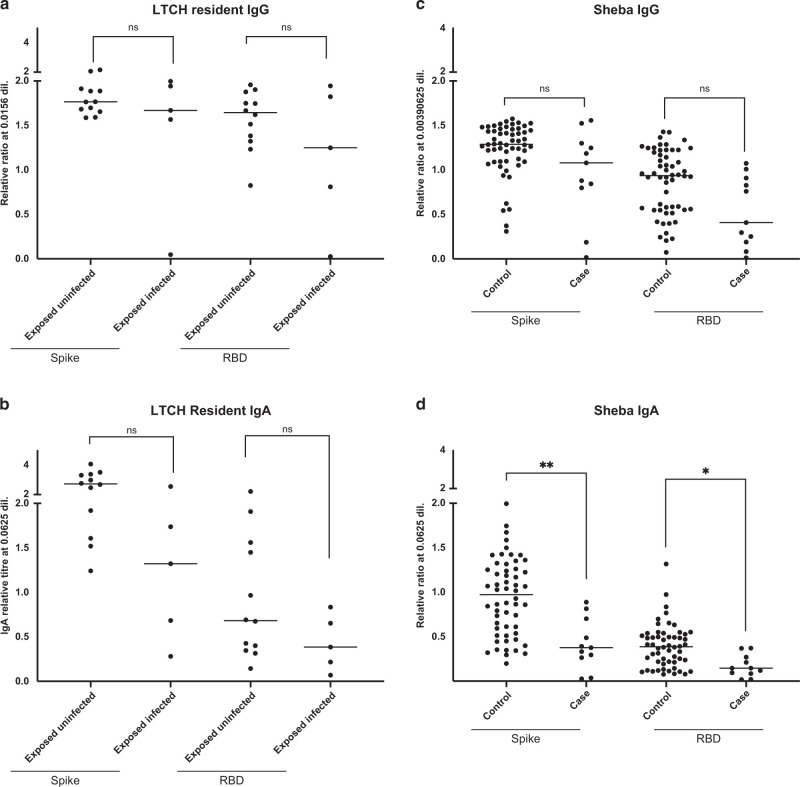
Although SARS-CoV-2 infects the upper respiratory tract, we know little about the amount, type, and kinetics of antibodies (Ab) generated in the oral cavity in response to COVID-19 vaccination. We collected serum and saliva samples from participants receiving two doses of mRNA COVID-19 vaccines and measured the level of anti-SARS-CoV-2 Ab. We detected anti-Spike and anti-Receptor Binding Domain (RBD) IgG and IgA, as well as anti-Spike/RBD associated secretory component in the saliva of most participants after dose 1. Administration of a second dose of mRNA boosted the IgG but not the IgA response, with only 30% of participants remaining positive for IgA at this timepoint. At 6 months post-dose 2, these participants exhibited diminished anti-Spike/RBD IgG levels, although secretory component-associated anti-Spike Ab were more stable. Examining two prospective cohorts we found that participants who experienced breakthrough infections with SARS-CoV-2 variants had lower levels of vaccine-induced serum anti-Spike/RBD IgA at 2-4 weeks post-dose 2 compared to participants who did not experience an infection, whereas IgG levels were comparable between groups. These data suggest that COVID-19 vaccines that elicit a durable IgA response may have utility in preventing infection. Our study finds that a local secretory component-associated IgA response is induced by COVID-19 mRNA vaccination that persists in some, but not all participants. The serum and saliva IgA response modestly correlate at 2-4 weeks post-dose 2. Of note, levels of anti-Spike serum IgA (but not IgG) at this timepoint are lower in participants who subsequently become infected with SARS-CoV-2. As new surges of SARS-CoV-2 variants arise, developing COVID-19 booster shots that provoke high levels of IgA has the potential to reduce person-to-person transmission.
© 2022. The Author(s), under exclusive licence to Society for Mucosal Immunology.
Conflict of interest statement
The authors declare no competing interests.
Figures




References
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
