

Microcirculatory Function in Nonhypertrophic and Hypertrophic Myocardium in Patients With Aortic Valve Stenosis
- PMID: 35470693
- PMCID: PMC9238586
- DOI: 10.1161/JAHA.122.025381
Microcirculatory Function in Nonhypertrophic and Hypertrophic Myocardium in Patients With Aortic Valve Stenosis
Abstract
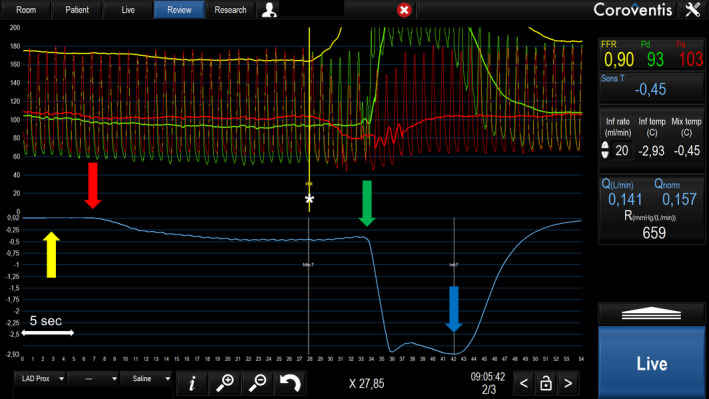
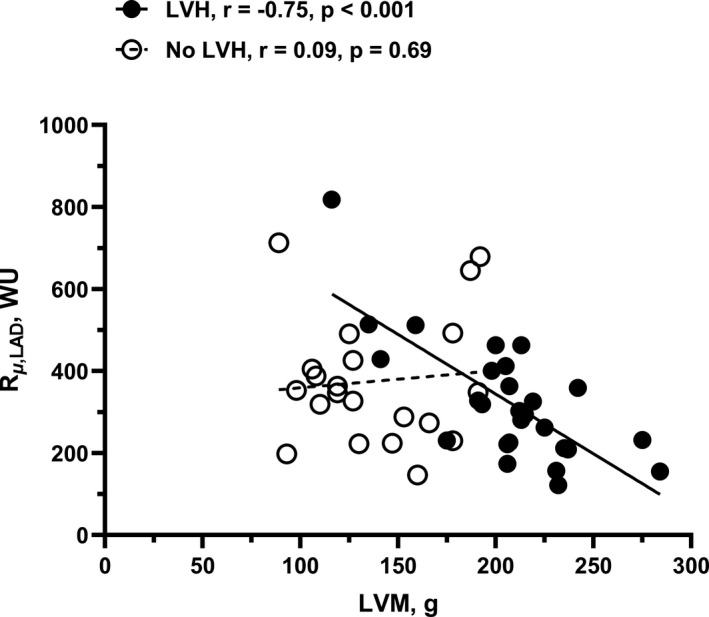
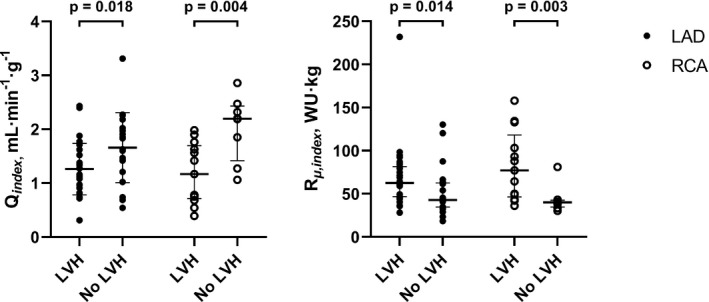
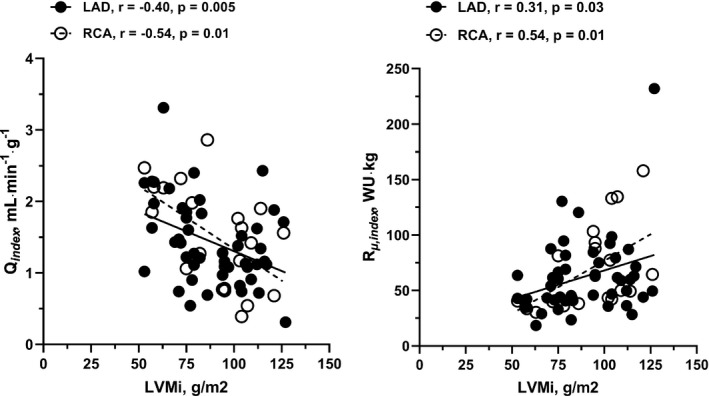
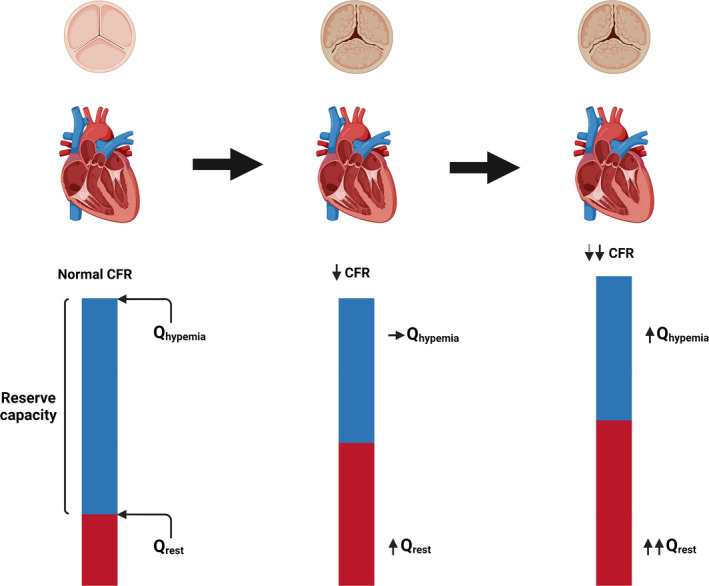
Background Left ventricular hypertrophy (LVH) has often been supposed to be associated with abnormal myocardial blood flow and resistance. The aim of this study was to evaluate and quantify the physiological and pathological changes in myocardial blood flow and microcirculatory resistance in patients with and without LVH attributable to severe aortic stenosis. Methods and Results Absolute coronary blood flow and microvascular resistance were measured using a novel technique with continuous thermodilution and infusion of saline. In addition, myocardial mass was assessed with cardiac magnetic resonance imaging. Fifty-three patients with aortic valve stenosis were enrolled in the study. In 32 patients with LVH, hyperemic blood flow per gram of tissue was significantly decreased compared with 21 patients without LVH (1.26±0.48 versus 1.66±0.65 mL·min-1·g-1; P=0.018), whereas minimal resistance indexed for left ventricular mass was significantly increased in patients with LVH (63 [47-82] versus 43 [35-63] Wood Units·kg; P=0.014). Conclusions Patients with LVH attributable to severe aortic stenosis had lower hyperemic blood flow per gram of myocardium and higher minimal myocardial resistance compared with patients without LVH.
Keywords: aortic stenosis; cardiac magnetic resonance imaging; coronary flow; left ventricular hypertrophy; microvascular function; thermodilution.
Figures
References
-
- Beach JM, Mihaljevic T, Rajeswaran J, Marwick T, Edwards ST, Nowicki ER, Thomas J, Svensson LG, Griffin B, Gillinov AM, et al. Ventricular hypertrophy and left atrial dilatation persist and are associated with reduced survival after valve replacement for aortic stenosis. J Thorac Cardiovasc Surg. 2014;147:362–369.e8. doi: 10.1016/j.jtcvs.2012.12.016 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
