

Outcome Prediction in Patients with Severe Traumatic Brain Injury Using Deep Learning from Head CT Scans
- PMID: 35471108
- PMCID: PMC9340242
- DOI: 10.1148/radiol.212181
Outcome Prediction in Patients with Severe Traumatic Brain Injury Using Deep Learning from Head CT Scans
Abstract
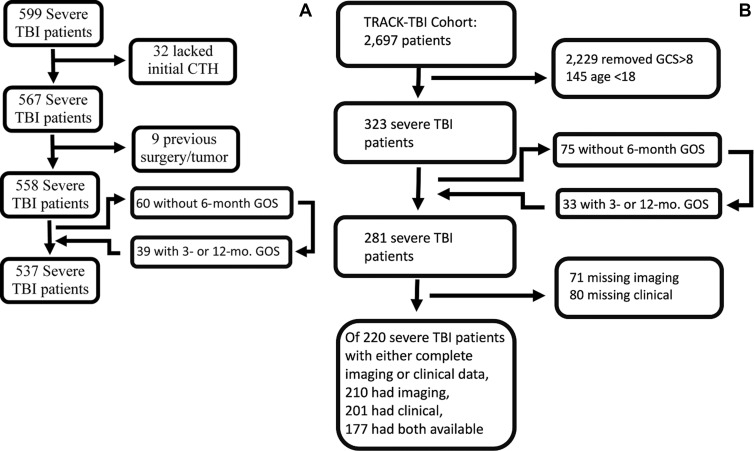
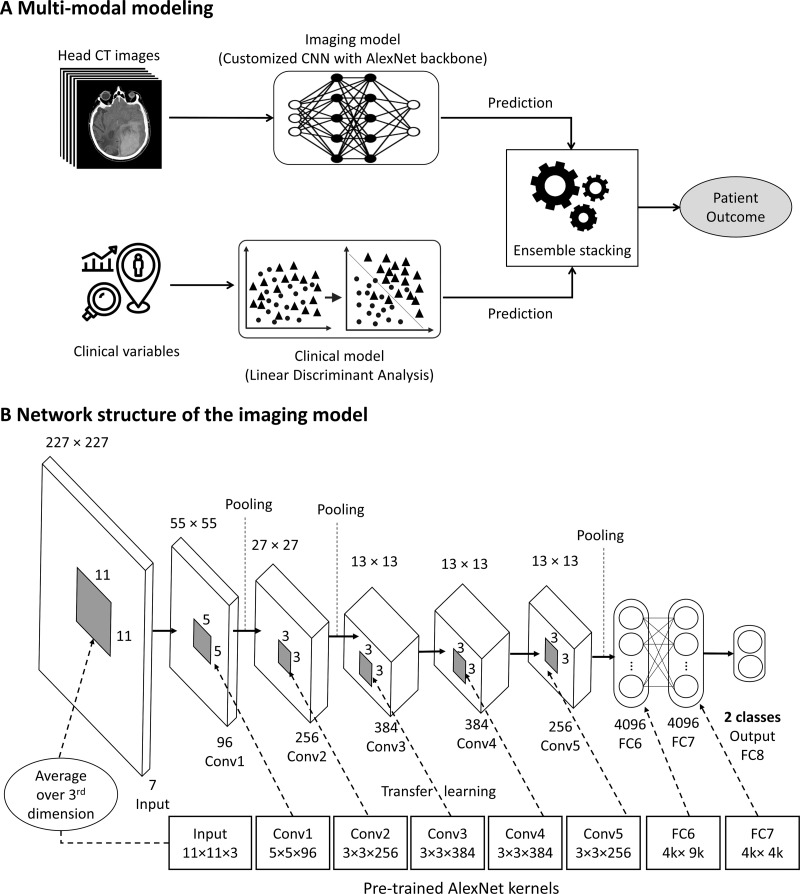
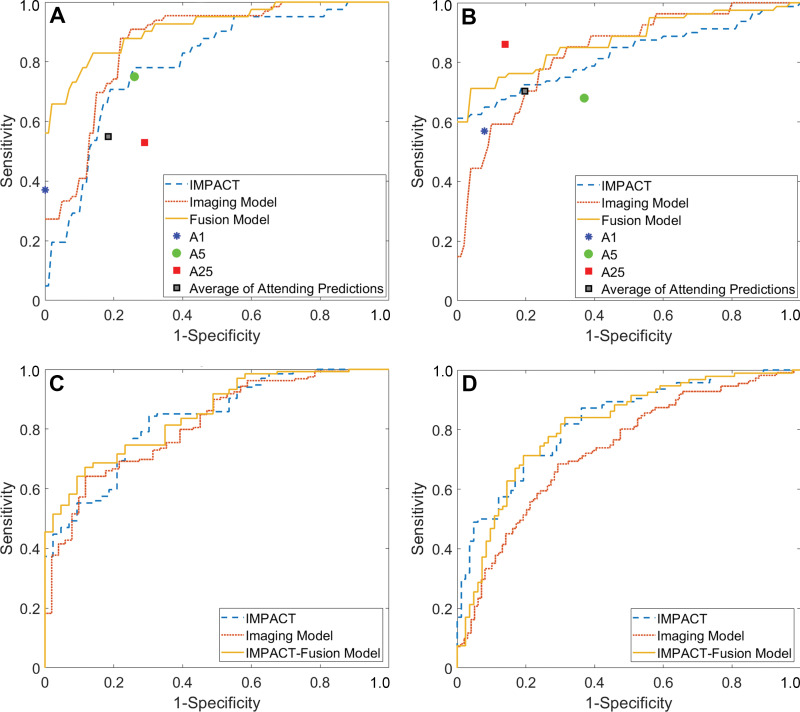
Background After severe traumatic brain injury (sTBI), physicians use long-term prognostication to guide acute clinical care yet struggle to predict outcomes in comatose patients. Purpose To develop and evaluate a prognostic model combining deep learning of head CT scans and clinical information to predict long-term outcomes after sTBI. Materials and Methods This was a retrospective analysis of two prospectively collected databases. The model-building set included 537 patients (mean age, 40 years ± 17 [SD]; 422 men) from one institution from November 2002 to December 2018. Transfer learning and curriculum learning were applied to a convolutional neural network using admission head CT to predict mortality and unfavorable outcomes (Glasgow Outcomes Scale scores 1-3) at 6 months. This was combined with clinical input for a holistic fusion model. The models were evaluated using an independent internal test set and an external cohort of 220 patients with sTBI (mean age, 39 years ± 17; 166 men) from 18 institutions in the Transforming Research and Clinical Knowledge in Traumatic Brain Injury (TRACK-TBI) study from February 2014 to April 2018. The models were compared with the International Mission on Prognosis and Analysis of Clinical Trials in TBI (IMPACT) model and the predictions of three neurosurgeons. Area under the receiver operating characteristic curve (AUC) was used as the main model performance metric. Results The fusion model had higher AUCs than did the IMPACT model in the prediction of mortality (AUC, 0.92 [95% CI: 0.86, 0.97] vs 0.80 [95% CI: 0.71, 0.88]; P < .001) and unfavorable outcomes (AUC, 0.88 [95% CI: 0.82, 0.94] vs 0.82 [95% CI: 0.75, 0.90]; P = .04) on the internal data set. For external TRACK-TBI testing, there was no evidence of a significant difference in the performance of any models compared with the IMPACT model (AUC, 0.83; 95% CI: 0.77, 0.90) in the prediction of mortality. The Imaging model (AUC, 0.73; 95% CI: 0.66-0.81; P = .02) and the fusion model (AUC, 0.68; 95% CI: 0.60, 0.76; P = .02) underperformed as compared with the IMPACT model (AUC, 0.83; 95% CI: 0.77, 0.89) in the prediction of unfavorable outcomes. The fusion model outperformed the predictions of the neurosurgeons. Conclusion A deep learning model of head CT and clinical information can be used to predict 6-month outcomes after severe traumatic brain injury. © RSNA, 2022 Online supplemental material is available for this article. See also the editorial by Haller in this issue.
Conflict of interest statement
Figures
Comment in
-
Deep Learning to Predict Outcome in Severe Traumatic Brain Injury.Radiology. 2022 Aug;304(2):395-396. doi: 10.1148/radiol.220412. Epub 2022 Apr 26. Radiology. 2022. PMID: 35471115 No abstract available.
References
-
- Centers for Disease Control and Prevention . Report to Congress on Traumatic Brain Injury in the United States: Epidemiology and Rehabilitation . National Center for Injury Prevention and Control; Division of Unintentional Injury Prevention. Atlanta, Ga: : Centers for Disease Control and Prevention, 2015. . - PubMed
-
- Myburgh JA, Cooper DJ, Finfer SR, et al. Epidemiology and 12-month outcomes from traumatic brain injury in Australia and New Zealand. J Trauma 2008;64(4):854–862. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
