

Quantitative CT Characteristics of Cluster Phenotypes in the Severe Asthma Research Program Cohorts
- PMID: 35471111
- PMCID: PMC9340243
- DOI: 10.1148/radiol.210363
Quantitative CT Characteristics of Cluster Phenotypes in the Severe Asthma Research Program Cohorts
Abstract
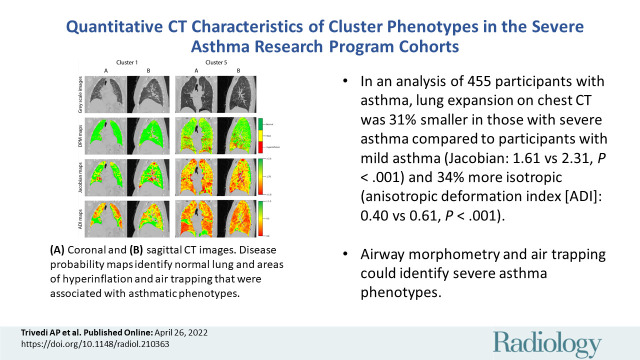
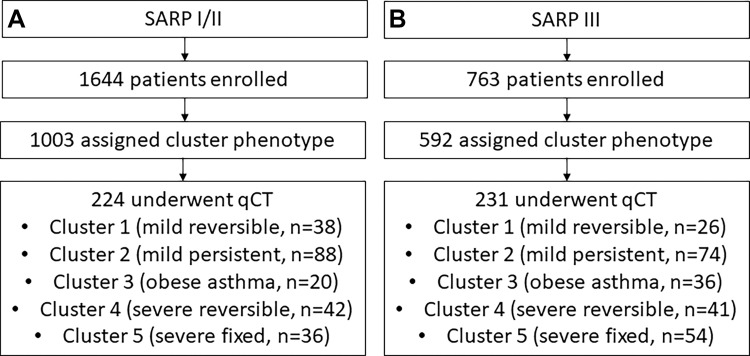
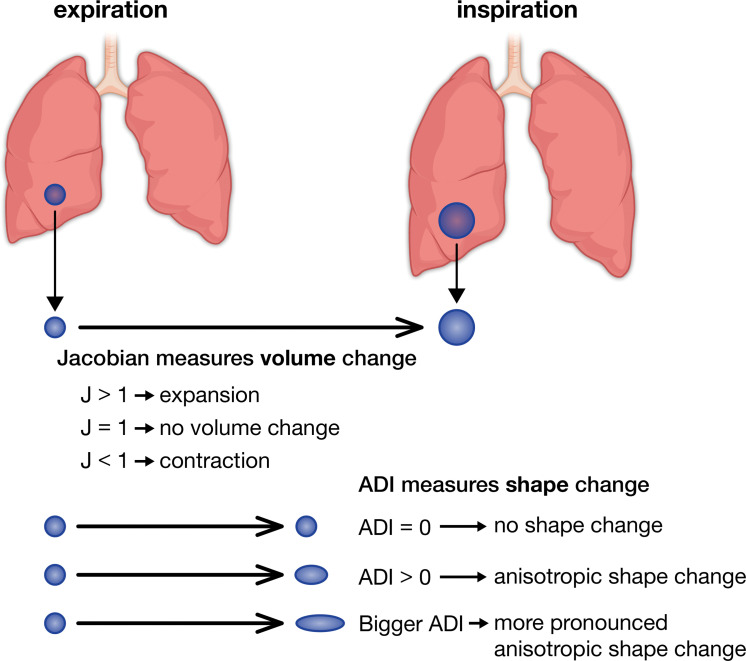
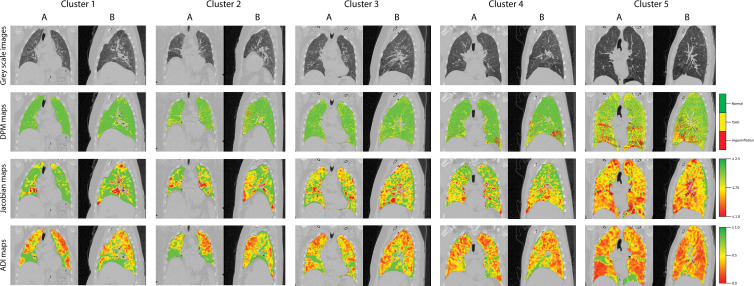
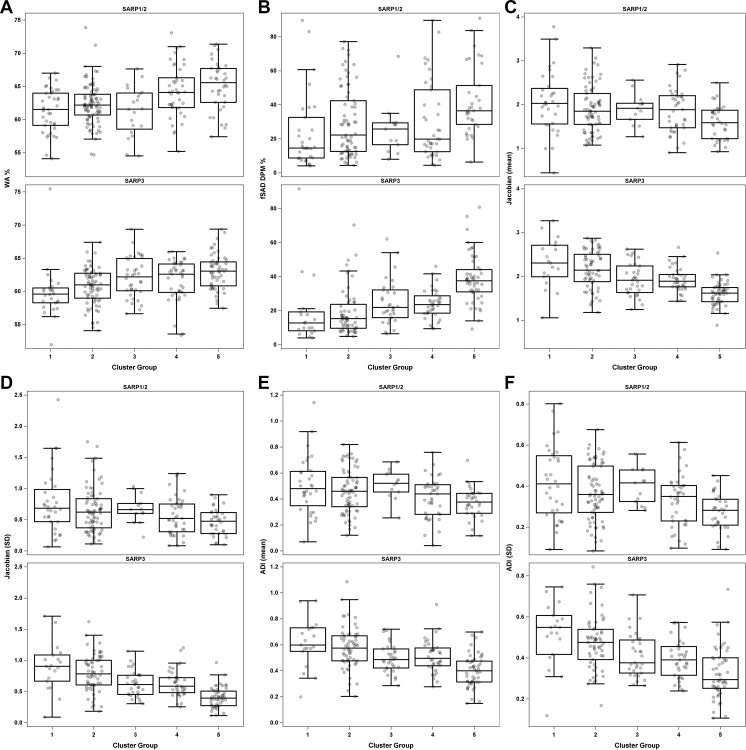
Background Clustering key clinical characteristics of participants in the Severe Asthma Research Program (SARP), a large, multicenter prospective observational study of patients with asthma and healthy controls, has led to the identification of novel asthma phenotypes. Purpose To determine whether quantitative CT (qCT) could help distinguish between clinical asthma phenotypes. Materials and Methods A retrospective cross-sectional analysis was conducted with the use of qCT images (maximal bronchodilation at total lung capacity [TLC], or inspiration, and functional residual capacity [FRC], or expiration) from the cluster phenotypes of SARP participants (cluster 1: minimal disease; cluster 2: mild, reversible; cluster 3: obese asthma; cluster 4: severe, reversible; cluster 5: severe, irreversible) enrolled between September 2001 and December 2015. Airway morphometry was performed along standard paths (RB1, RB4, RB10, LB1, and LB10). Corresponding voxels from TLC and FRC images were mapped with use of deformable image registration to characterize disease probability maps (DPMs) of functional small airway disease (fSAD), voxel-level volume changes (Jacobian), and isotropy (anisotropic deformation index [ADI]). The association between cluster assignment and qCT measures was evaluated using linear mixed models. Results A total of 455 participants were evaluated with cluster assignments and CT (mean age ± SD, 42.1 years ± 14.7; 270 women). Airway morphometry had limited ability to help discern between clusters. DPM fSAD was highest in cluster 5 (cluster 1 in SARP III: 19.0% ± 20.6; cluster 2: 18.9% ± 13.3; cluster 3: 24.9% ± 13.1; cluster 4: 24.1% ± 8.4; cluster 5: 38.8% ± 14.4; P < .001). Lower whole-lung Jacobian and ADI values were associated with greater cluster severity. Compared to cluster 1, cluster 5 lung expansion was 31% smaller (Jacobian in SARP III cohort: 2.31 ± 0.6 vs 1.61 ± 0.3, respectively, P < .001) and 34% more isotropic (ADI in SARP III cohort: 0.40 ± 0.1 vs 0.61 ± 0.2, P < .001). Within-lung Jacobian and ADI SDs decreased as severity worsened (Jacobian SD in SARP III cohort: 0.90 ± 0.4 for cluster 1; 0.79 ± 0.3 for cluster 2; 0.62 ± 0.2 for cluster 3; 0.63 ± 0.2 for cluster 4; and 0.41 ± 0.2 for cluster 5; P < .001). Conclusion Quantitative CT assessments of the degree and intraindividual regional variability of lung expansion distinguished between well-established clinical phenotypes among participants with asthma from the Severe Asthma Research Program study. © RSNA, 2022 Online supplemental material is available for this article. See also the editorial by Verschakelen in this issue.
Conflict of interest statement
Figures
Comment in
-
Quantitative CT of the Lung to Study Asthma.Radiology. 2022 Aug;304(2):460-461. doi: 10.1148/radiol.213091. Epub 2022 Apr 26. Radiology. 2022. PMID: 35471116 No abstract available.
References
-
- Nurmagambetov T , Kuwahara R , Garbe P . The Economic Burden of Asthma in the United States, 2008-2013 . Ann Am Thorac Soc 2018. ; 15 ( 3 ): 348– 356 . - PubMed
-
- Hekking PW , Wener RR , Amelink M , Zwinderman AH , Bouvy ML , Bel EH . The prevalence of severe refractory asthma . J Allergy Clin Immunol 2015. ; 135 ( 4 ): 896– 902 . - PubMed
-
- Ivanova JI , Bergman R , Birnbaum HG , Colice GL , Silverman RA , McLaurin K . Effect of asthma exacerbations on health care costs among asthmatic patients with moderate and severe persistent asthma . J Allergy Clin Immunol 2012. ; 129 ( 5 ): 1229– 1235 . - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
