

Physicians' misperceived cardiovascular risk and therapeutic inertia as determinants of low LDL-cholesterol targets achievement in diabetes
- PMID: 35473579
- PMCID: PMC9044595
- DOI: 10.1186/s12933-022-01495-8
Physicians' misperceived cardiovascular risk and therapeutic inertia as determinants of low LDL-cholesterol targets achievement in diabetes
Erratum in
-
Correction to: Physicians' misperceived cardiovascular risk and therapeutic inertia as determinants of low LDL-cholesterol targets achievement in diabetes.Cardiovasc Diabetol. 2022 May 13;21(1):73. doi: 10.1186/s12933-022-01515-7. Cardiovasc Diabetol. 2022. PMID: 35562766 Free PMC article. No abstract available.
Abstract
Background: Greater efforts are needed to overcome the worldwide reported low achievement of LDL-c targets. This survey aimed to dissect whether and how the physician-based evaluation of patients with diabetes is associated with the achievement of LDL-c targets.
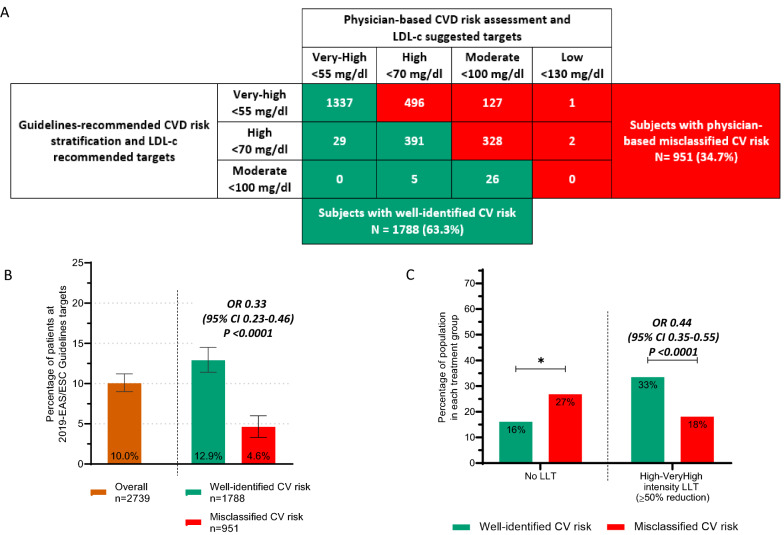
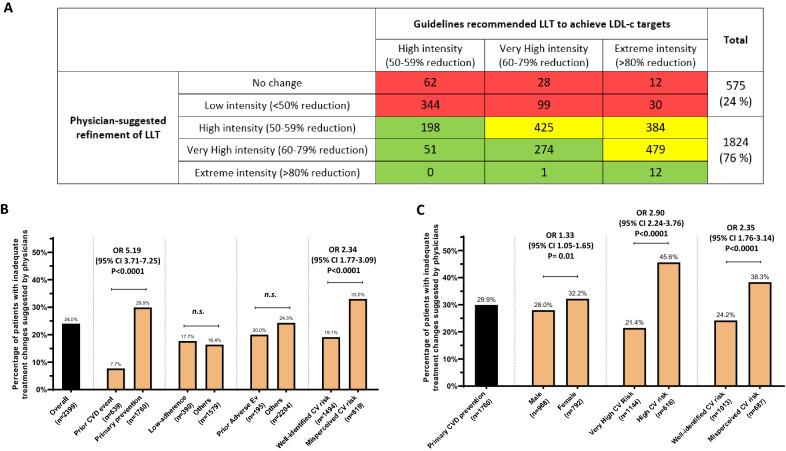
Methods: This cross-sectional self-reported survey interviewed physicians working in 67 outpatient services in Italy, collecting records on 2844 patients with diabetes. Each physician reported a median of 47 records (IQR 42-49) and, for each of them, the physician specified its perceived cardiovascular risk, LDL-c targets, and the suggested refinement in lipid-lowering-treatment (LLT). These physician-based evaluations were then compared to recommendations from EAS/EASD guidelines.
Results: Collected records were mostly from patients with type 2 diabetes (94%), at very-high (72%) or high-cardiovascular risk (27%). Physician-based assessments of cardiovascular risk and of LDL-c targets, as compared to guidelines recommendation, were misclassified in 34.7% of the records. The misperceived assessment was significantly higher among females and those on primary prevention and was associated with 67% lower odds of achieving guidelines-recommended LDL-c targets (OR 0.33, p < 0.0001). Peripheral artery disease, target organ damage and LLT-initiated by primary-care-physicians were all factors associated with therapeutic-inertia (i.e., lower than expected probability of receiving high-intensity LLT). Physician-suggested LLT refinement was inadequate in 24% of overall records and increased to 38% among subjects on primary prevention and with misclassified cardiovascular risk.
Conclusions: This survey highlights the need to improve the physicians' misperceived cardiovascular risk and therapeutic inertia in patients with diabetes to successfully implement guidelines recommendations into everyday clinical practice.
Keywords: Adherence; Cardiovascular risk; Ezetimibe; Inertia; Misperceived risk; PCSK9i; Primary care physicians; Real-world; Real-world study; Self-reported survey; Statins.
© 2022. The Author(s).
Conflict of interest statement
MLM received lecture or advisory fees or grant support from Mylan, SlaPharma, Servier, Lilly, MSD, Novo Nordisk, and was unconditionally supported by LatoC Srl for conducting the analyses of the data of the current work and writing the manuscript. OL received speaker or advisory board fees from Eli-Lilly and NovoNordisk, research grants from Astra Zeneca. EM none. AG has received honoraria or consulting fees from Amgen, AstraZeneca, Boehringer Ingelheim, Eli Lilly, MSD, and Sanofi, and research funding from AstraZeneca. AA received research grants, lecture or advisory board fees from Merck Sharp & Dome, AstraZeneca, Novartis, Boeringher-Ingelheim, Sanofi, Mediolanum, Janssen, Novo Nordisk, Lilly, Servier, and Takeda.
Figures

References
-
- Bruckert E, Parhofer KG, Gonzalez-Juanatey JR, Nordestgaard B, Arca M, Giovas P, et al. Proportion of high-risk/very high-risk patients in Europe with low-density lipoprotein cholesterol at target according to European guidelines: a systematic review. Adv Ther. 2020;37(5):1724–1736. doi: 10.1007/s12325-020-01285-2. - DOI - PMC - PubMed
-
- Morieri ML, Perrone V, Veronesi C, Degli Esposti L, Andretta M, Plebani M, et al. Improving statin treatment strategies to reduce LDL-cholesterol: factors associated with targets' attainment in subjects with and without type 2 diabetes. Cardiovasc Diabetol. 2021;20(1):144. doi: 10.1186/s12933-021-01338-y. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
