

Risk factors of pacing dependence and cardiac dysfunction in patients with permanent pacemaker implantation
- PMID: 35474306
- PMCID: PMC9288795
- DOI: 10.1002/ehf2.13918
Risk factors of pacing dependence and cardiac dysfunction in patients with permanent pacemaker implantation
Abstract
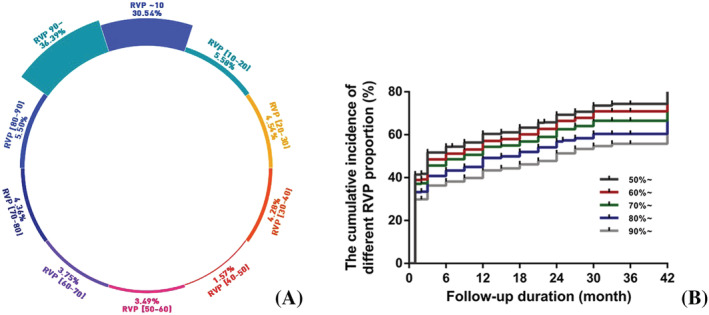
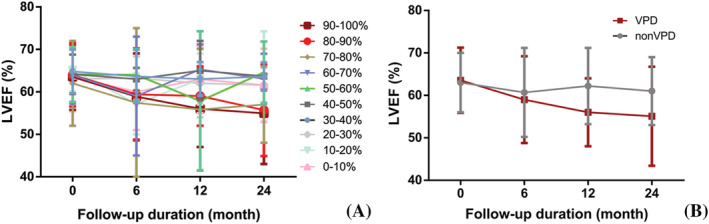
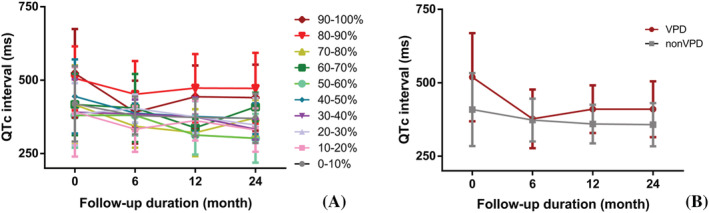
Aims: Right ventricular pacing (RVP) dependence could impair left ventricular ejection fraction (LVEF). This study aimed to illuminate the relationship between RVP proportion and LVEF, as well as disclosing independent predictors of RVP dependence.
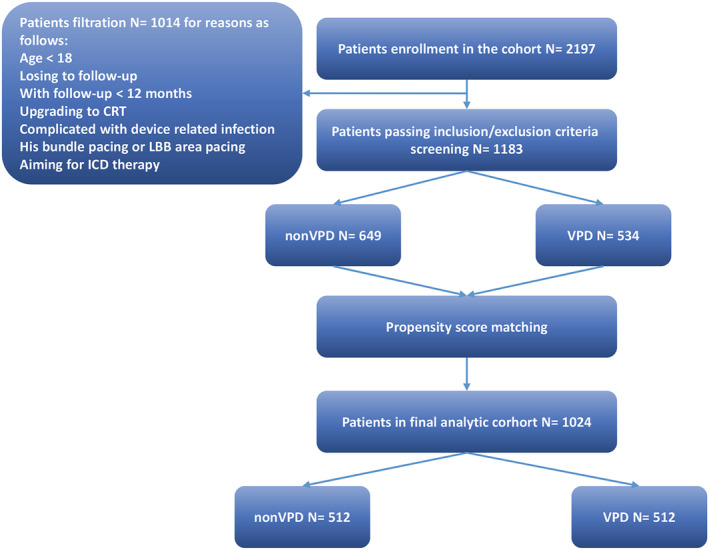
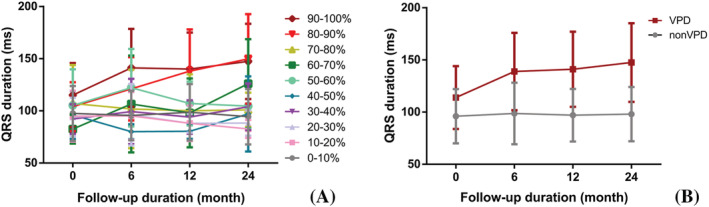
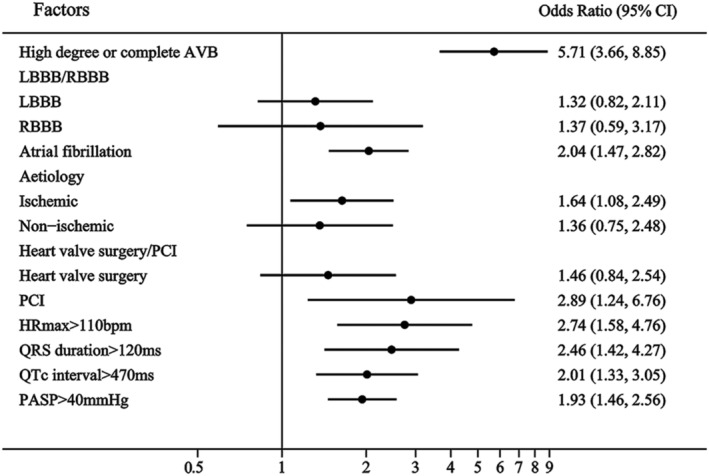
Methods and results: Patients indicated for permanent pacemaker implantation were included (2016-2020). The ventricular pacing lead was placed in right ventricular apex or septum. Pacing mode programming followed universal standard. Electrocardiographic, echocardiographic, and serological parameters were collected. RVP dependence was defined according to its influence on LVEF. This study was of case-control design. Included patients were matched by potentially confounding factors through propensity score matching. A total of 1183 patients were included, and the mean duration of follow-up was 24 months. Percentage of RVP < 80% hardly influenced LVEF; however, LVEF tended to decrease with higher RVP proportion. High degree/complete atrioventricular block (AVB) [odds ratio (OR) = 5.71, 95% confidence interval (CI): 3.66-8.85], atrial fibrillation (AF) (OR = 2.04, 95% CI: 1.47-2.82), percutaneous coronary intervention (PCI) (OR = 2.89, 95% CI: 1.24-6.76), maximum heart rate (HRmax ) < 110 b.p.m. (OR = 2.74, 95% CI: 1.58-4.76), QRS duration > 120 ms (OR = 2.46, 95% CI: 1.42-4.27), QTc interval > 470 ms (OR = 2.01, 95% CI: 1.33-3.05), and pulmonary artery systolic pressure (PASP) > 40 mmHg (OR = 1.93, 95% CI: 1.46-2.56) were proved to predict RVP dependence.
Conclusions: High RVP percentage (>80%) indicating RVP dependence significantly correlates with poor prognosis of cardiac function. High degree/complete AVB, AF, ischaemic aetiology, PCI history, HRmax < 110 b.p.m., QRS duration > 120 ms, QTc interval > 470 ms, and PASP > 40 mmHg were verified as independent risk factors of RVP dependence.
Keywords: Cardiac dysfunction; Pacemaker; Pacing dependence; Right ventricular pacing.
© 2022 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
Similar articles
-
Impact of Physiologic Pacing Versus Right Ventricular Pacing Among Patients With Left Ventricular Ejection Fraction Greater Than 35%: A Systematic Review for the 2018 ACC/AHA/HRS Guideline on the Evaluation and Management of Patients With Bradycardia and Cardiac Conduction Delay: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society.Circulation. 2019 Aug 20;140(8):e483-e503. doi: 10.1161/CIR.0000000000000629. Epub 2018 Nov 6. Circulation. 2019. PMID: 30586773
-
Left Bundle Branch Area Pacing Versus Right Ventricular Pacing in Patients With Atrioventricular Block: A Systematic Review and Meta-Analysis.J Cardiovasc Electrophysiol. 2025 Feb;36(2):501-511. doi: 10.1111/jce.16548. Epub 2025 Jan 7. J Cardiovasc Electrophysiol. 2025. PMID: 39775893 Free PMC article.
-
Impact of Physiologic Pacing Versus Right Ventricular Pacing Among Patients With Left Ventricular Ejection Fraction Greater Than 35%: A Systematic Review for the 2018 ACC/AHA/HRS Guideline on the Evaluation and Management of Patients With Bradycardia and Cardiac Conduction Delay: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society.J Am Coll Cardiol. 2019 Aug 20;74(7):988-1008. doi: 10.1016/j.jacc.2018.10.045. Epub 2018 Nov 6. J Am Coll Cardiol. 2019. PMID: 30412708
-
[Left atrial and ventricular epicardial dual chamber pacing through a left lateral thoracotomy to treat pediatric complete atrioventricular block].Zhonghua Er Ke Za Zhi. 2013 Aug;51(8):578-83. Zhonghua Er Ke Za Zhi. 2013. PMID: 24225287 Chinese.
-
New-onset atrial high-rate episodes in left bundle branch area pacing versus right ventricular pacing for patients with atrioventricular block.Kardiol Pol. 2024;82(6):632-639. doi: 10.33963/v.phj.100403. Epub 2024 May 7. Kardiol Pol. 2024. PMID: 38712772
Cited by
-
Prognosis of pacing-dependent patients with cardiovascular implantable electronic devices.Herzschrittmacherther Elektrophysiol. 2024 Mar;35(1):39-45. doi: 10.1007/s00399-024-00996-1. Epub 2024 Jan 31. Herzschrittmacherther Elektrophysiol. 2024. PMID: 38294518 Free PMC article.
-
Clinical value of the fibrosis-4 index in predicting mortality in patients with right ventricular pacing.PLoS One. 2024 Feb 5;19(2):e0294221. doi: 10.1371/journal.pone.0294221. eCollection 2024. PLoS One. 2024. PMID: 38315703 Free PMC article.
References
-
- Catanzariti D, Maines M, Manica A, Angheben C, Varbaro A, Vergara G. Permanent His‐bundle pacing maintains long‐term ventricular synchrony and left ventricular performance, unlike conventional right ventricular apical pacing. Europace. 2013; 15: 546–553. - PubMed
-
- Slotwiner DJ, Raitt MH, Del‐Carpio MF, Mulpuru SK, Nasser N, Peterson PN. Impact of physiologic pacing versus right ventricular pacing among patients with left ventricular ejection fraction greater than 35%: a systematic review for the 2018 ACC/AHA/HRS guideline on the evaluation and management of patients with bradycardia and cardiac conduction delay: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Circulation. 2019; 140: e483–e503. - PubMed
-
- Pastore G, Zanon F, Baracca E, Aggio S, Corbucci G, Boaretto G, Roncon L, Noventa F, Barold SS. The risk of atrial fibrillation during right ventricular pacing. Europace. 2016; 18: 353–358. - PubMed
-
- Silberbauer J, Veasey RA, Freemantle N, Arya A, Boodhoo L, Sulke N. The relationship between high‐frequency right ventricular pacing and paroxysmal atrial fibrillation burden. Europace. 2009; 11: 1456–1461. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
