

Risk factors and medical resource utilization in US adults hospitalized with influenza or respiratory syncytial virus in the Hospitalized Acute Respiratory Tract Infection study
- PMID: 35474419
- PMCID: PMC9343339
- DOI: 10.1111/irv.12994
Risk factors and medical resource utilization in US adults hospitalized with influenza or respiratory syncytial virus in the Hospitalized Acute Respiratory Tract Infection study
Abstract
Background: Influenza and respiratory syncytial virus (RSV) are associated with substantial morbidity and mortality in the United States. We assessed risk factors for severe disease and medical resource utilization (MRU) among US adults hospitalized with influenza or RSV in the Hospitalized Acute Respiratory Tract Infection (HARTI) study.
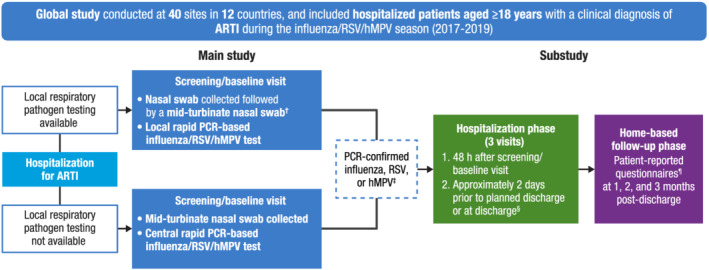
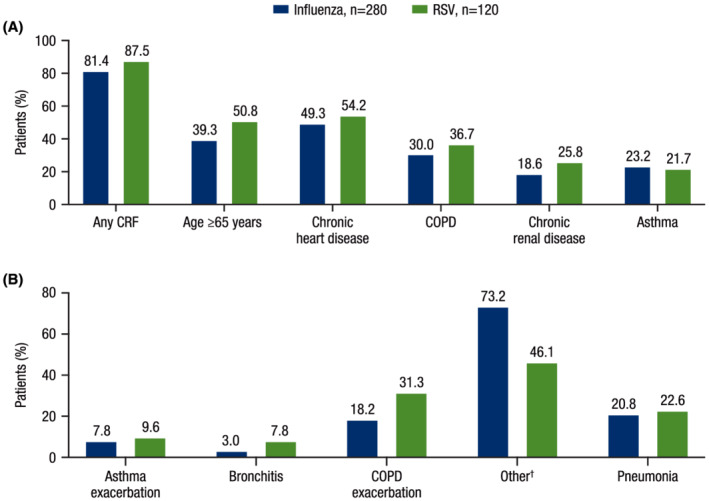
Methods: HARTI was a prospective global (40 centers, 12 countries) epidemiological study of adults hospitalized with acute respiratory tract infections conducted across the 2017-2019 epidemic seasons. Patients with confirmed influenza or RSV were followed up to 3 months post-discharge. Baseline characteristics, prevalence of core risk factors (CRFs) for severe disease (age ≥65 years, chronic heart or renal disease, chronic obstructive pulmonary disease, or asthma), and MRU were summarized descriptively.
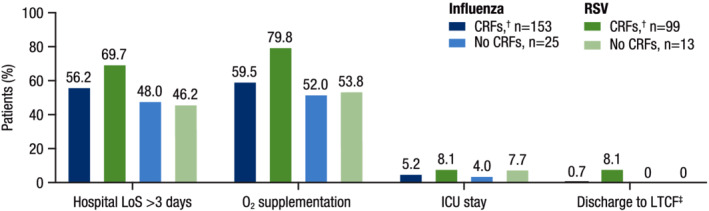
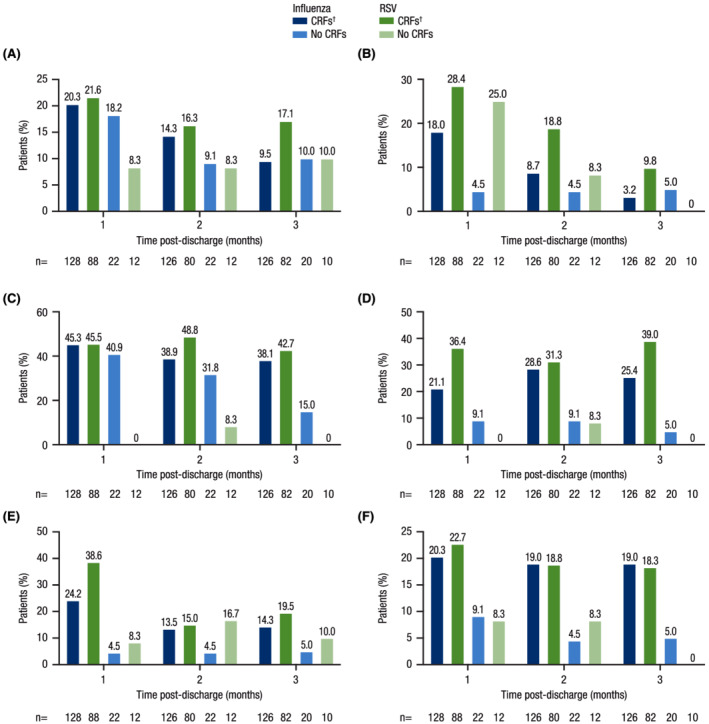
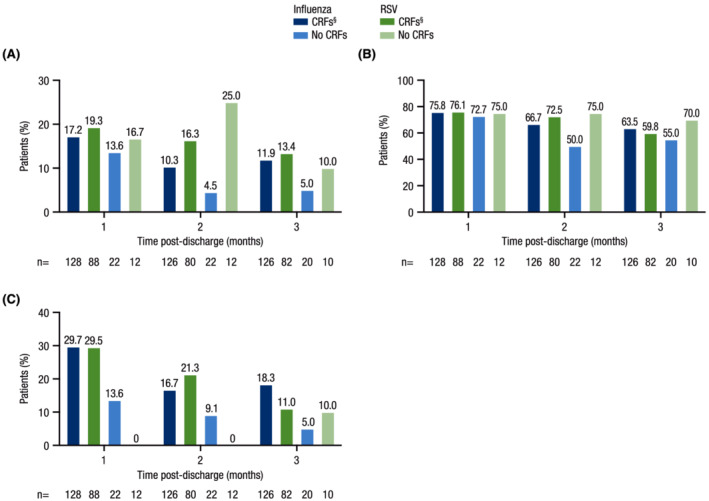
Results: The US cohort included 280 influenza-positive and 120 RSV-positive patients. RSV patients were older (mean: 63.1 vs. 59.7 years) and a higher proportion had CRFs (87.5% vs. 81.4%). Among those with CRFs (influenza, n = 153; RSV, n = 99), RSV patients required longer hospitalizations (median length of stay: 4.5 days) and a greater proportion (79.8%) required oxygen supplementation during hospitalization compared with influenza patients (4.0 days and 59.5%, respectively). At 3 months post-discharge, a greater proportion of RSV patients with CRFs reported use of antibiotics, antitussives, bronchodilators, and inhaled and systemic steroids versus those with influenza and CRFs. Many patients with CRFs reported hospital readmission at 3 months post-discharge (RSV: 13.4%; influenza: 11.9%).
Conclusions: MRU during and post-hospitalization due to RSV in adults is similar to or greater than that of influenza. Enhanced RSV surveillance and preventive and therapeutic interventions are needed.
Keywords: hospitalization; influenza; prospective study; respiratory infections; respiratory syncytial virus; risk factors.
© 2022 Janssen Scientific Affairs, LLC. Influenza and Other Respiratory Viruses published by John Wiley & Sons Ltd.
Figures
References
-
- GBD Lower Respiratory Infections Collaborators . Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory infections in 195 countries, 1990‐2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Infect Dis. 2018;18(11):1191‐1210. doi:10.1016/S1473-3099(18)30310-4 - DOI - PMC - PubMed
-
- World Health Organization . Global influenza strategy. 2019. https://www.who.int/publications/i/item/9789241515320. Accessed January 3, 2022.
-
- National Institutes of Health, National Institute of Allergy and Infectious Diseases . Respiratory syncytial virus (RSV). 2008. https://www.niaid.nih.gov/diseases-conditions/respiratory-syncytial-viru.... Accessed October 5, 2021.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
