

Dynamic change of mitral regurgitation after myocardial reverse remodelling: a case report
- PMID: 35474683
- PMCID: PMC9026222
- DOI: 10.1093/ehjcr/ytac110
Dynamic change of mitral regurgitation after myocardial reverse remodelling: a case report
Abstract
Background: Chronic mitral regurgitation can be primary (degenerative) or secondary (functional); each has its own aetiology, treatment approach, and prognosis. A combination of the two types of regurgitation can lead to unexpected haemodynamic changes.
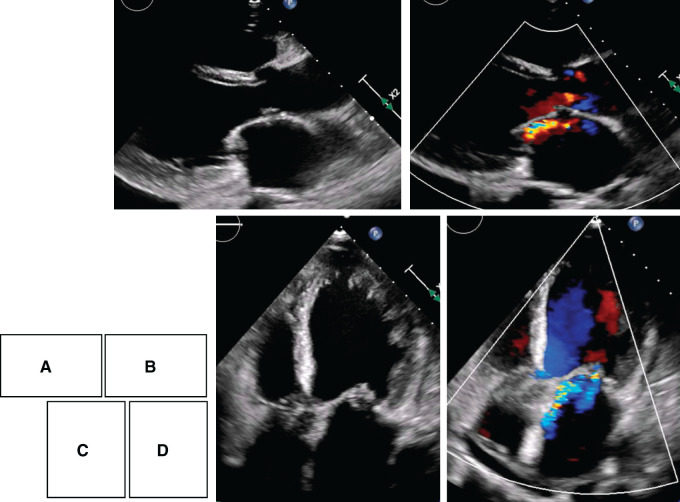
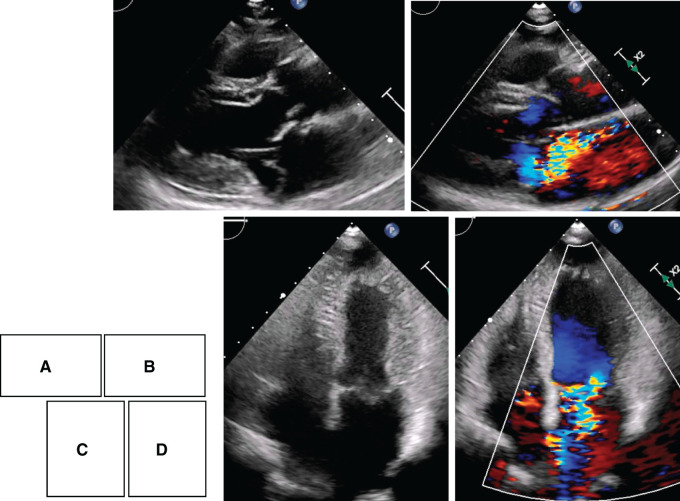
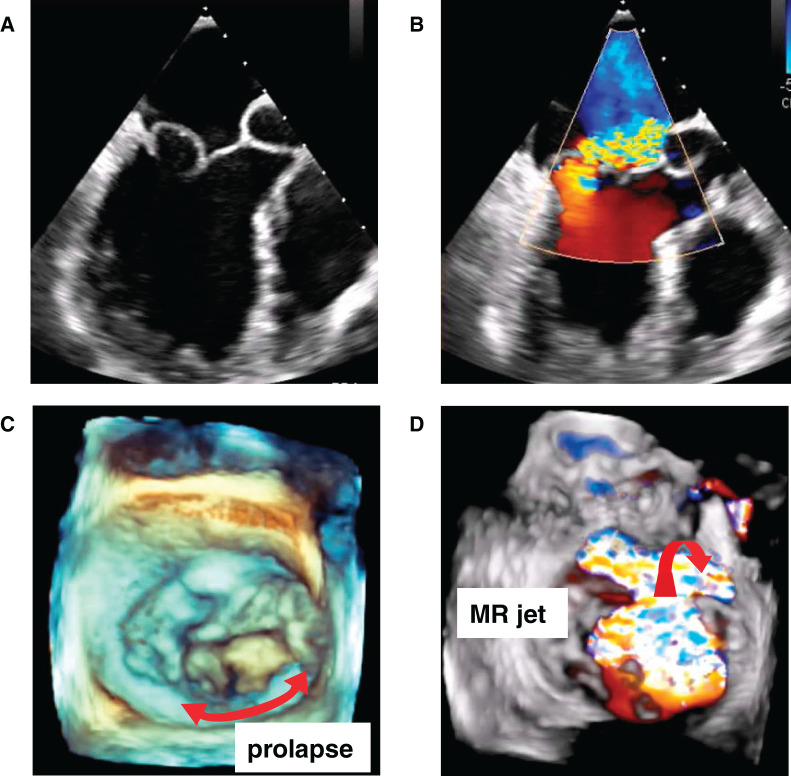
Case summary: A 72-year-old woman presented to our hospital with dyspnoea on exertion, moist cough, and orthopnoea. At admission, transthoracic echocardiography (TTE) findings revealed severely reduced left ventricular ejection fraction, dilation of the left ventricle and left atrium, mild mitral regurgitation with prolapse of the posterior leaflet, and bilateral leaflet tethering. She was diagnosed with idiopathic cardiomyopathy with mild mitral regurgitation. After compensation of heart failure, angiotensin-receptor blocker and beta-blocker treatment were initiated, and the dose was subsequently titrated. At 7 months after initiating medical therapy, TTE showed significant improvement of the left ventricular ejection fraction, disappearance of left ventricular dilation (reverse remodelling), and mitral valve tethering. However, posterior leaflet prolapse became apparent, and mitral regurgitation blowing became more severe. Chordal lengthening, leaflet thickening, and degeneration were observed, but there were no ruptured chordae. Successful surgical repair of the mitral and tricuspid valves was performed.
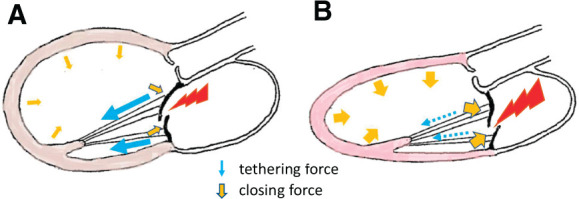
Discussion: In this unusual mitral regurgitation case, the regurgitation worsened following an improvement of cardiac function due to the loss of tethering from a reduction of the left ventricular diameter and an increase in closing force by increasing the left ventricular contractile force. Eventually, mitral regurgitation prolapse became apparent. Therefore, we should consider that reverse remodelling may exacerbate mitral regurgitation.
Keywords: Case report; Mitral regurgitation; Mitral valve tethering; Myocardial reverse remodelling; Prolapse.
© The Author(s) 2022. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures

Similar articles
-
Chordal translocation for ischemic mitral regurgitation may ameliorate tethering of the posterior and anterior mitral leaflets.J Thorac Cardiovasc Surg. 2008 Oct;136(4):868-75. doi: 10.1016/j.jtcvs.2008.06.034. J Thorac Cardiovasc Surg. 2008. PMID: 18954624
-
Efficacy of chordal cutting in alleviating ischemic mitral regurgitation: insights from 3-dimensional echocardiography.J Cardiothorac Surg. 2007 Sep 25;2:39. doi: 10.1186/1749-8090-2-39. J Cardiothorac Surg. 2007. PMID: 17894872 Free PMC article.
-
Left ventricular performance early after repair for posterior mitral leaflet prolapse: Chordal replacement versus leaflet resection.J Thorac Cardiovasc Surg. 2015 Sep;150(3):538-45. doi: 10.1016/j.jtcvs.2015.06.022. Epub 2015 Jun 18. J Thorac Cardiovasc Surg. 2015. PMID: 26189162
-
[Use of echocardiography in mitral regurgitation for the assessment of its mechanism and etiology for the morphological analysis of the mitral valve].Ann Cardiol Angeiol (Paris). 2003 Apr;52(2):70-7. doi: 10.1016/s0003-3928(03)00007-6. Ann Cardiol Angeiol (Paris). 2003. PMID: 12754963 Review. French.
-
The mechanisms, diagnosis and management of mitral regurgitation in mitral valve prolapse and hypertrophic cardiomyopathy.Discoveries (Craiova). 2016 Jun 30;4(2):e61. doi: 10.15190/d.2016.8. Discoveries (Craiova). 2016. PMID: 32309580 Free PMC article. Review.
References
-
- Baumgartner H, Falk V, Bax JJ, De Bonis M, Hamm C, Holm PJ. et al.; ESC Scientific Document Group. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J 2017;38:2739–2791. - PubMed
-
- Asgar AW, Mack MJ, Stone GW.. Secondary mitral regurgitation in heart failure: pathophysiology, prognosis, and therapeutic considerations. J Am Coll Cardiol 2015;65:1231–1248. - PubMed
-
- Carpentier A. Cardiac valve surgery—the “French correction”. J Thorac Cardiovasc Surg 1983;86:323–337. - PubMed
Publication types
LinkOut - more resources
Full Text Sources