

Mortality in men with castration-resistant prostate cancer-A long-term follow-up of a population-based real-world cohort
- PMID: 35474724
- PMCID: PMC8988790
- DOI: 10.1002/bco2.116
Mortality in men with castration-resistant prostate cancer-A long-term follow-up of a population-based real-world cohort
Abstract
Objectives: The objective of this study is to find clinical variables that predict the prognosis for men with castration-resistant prostate cancer (CRPC) in a Swedish real-life CRPC cohort, including a risk group classification to clarify the risk of succumbing to prostate cancer. This is a natural history cohort representing the premodern drug era before the introduction of novel hormonal drug therapies.
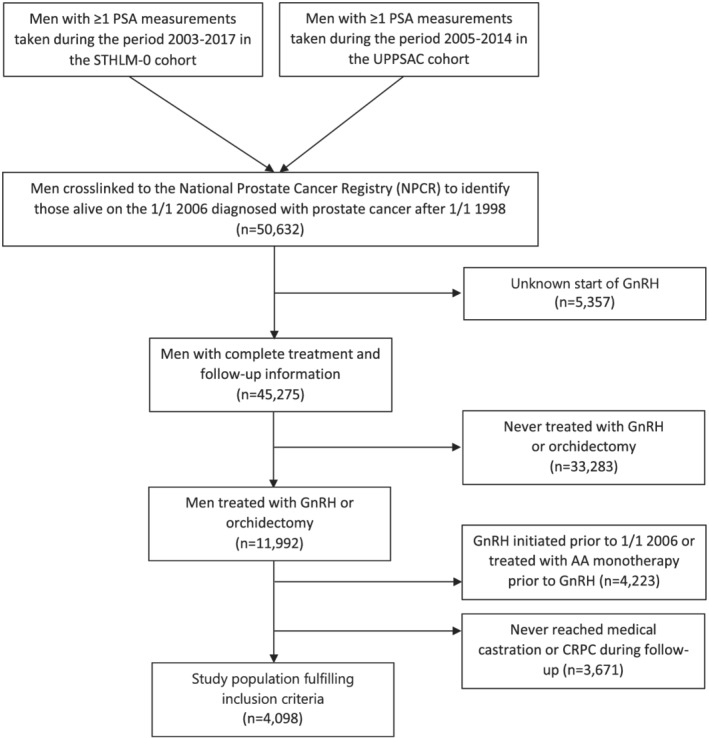
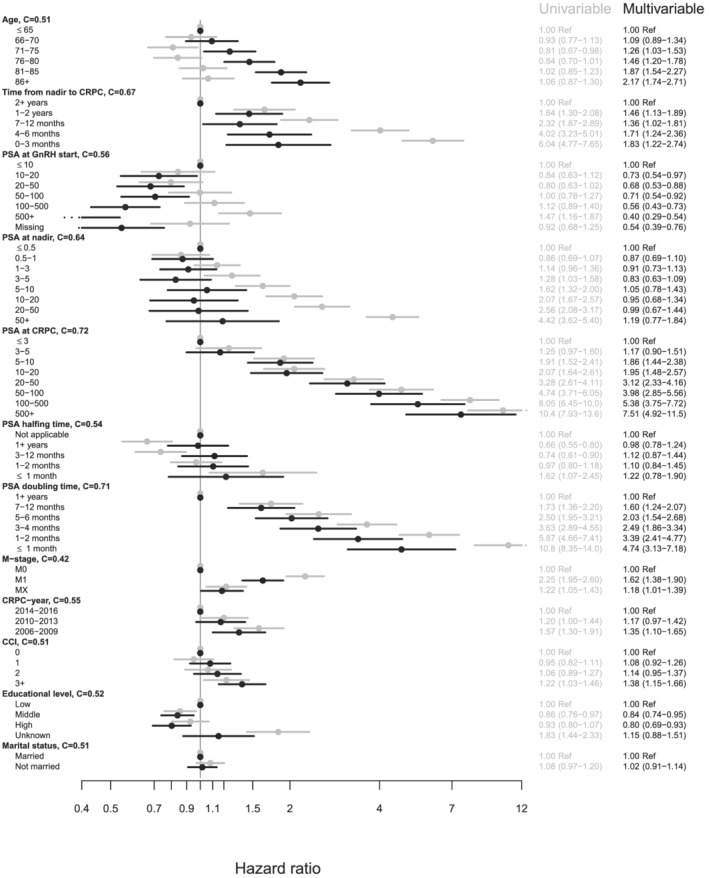
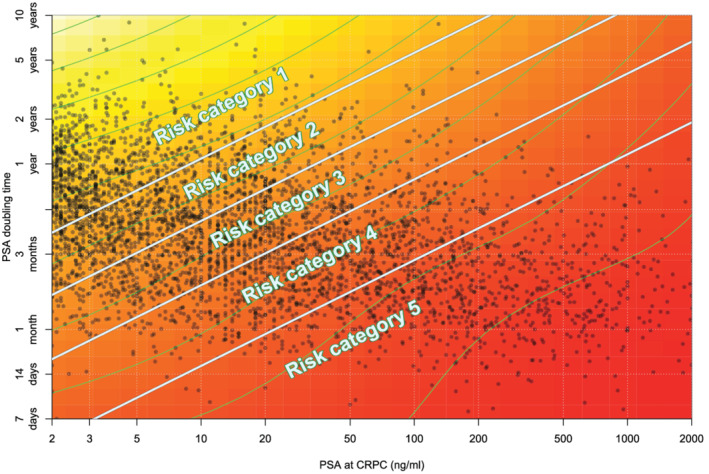
Methods: PSA tests from the clinical chemistry laboratories serving health care in six regions of Sweden were retrieved and cross-linked to the National Prostate Cancer Registry (NPCR) to identify men with a prostate cancer diagnosis. Through further cross-linking with data sources at the Swedish Board of Health and Welfare, we retrieved other relevant information such as prescribed drugs, hospitalizations, and cause of death. Men entered the CRPC cohort at the first date of doubling of their PSA nadir value with the last value being >2 ng/ml, or an absolute increase of >5 ng/ml or more, whilst on 3 months of medical castration or if they had been surgically castrated (n = 4098). By combining the two variables with the largest C-statistics, "PSA at time of CRPC" and "PSA doubling time," a risk group classification was created.
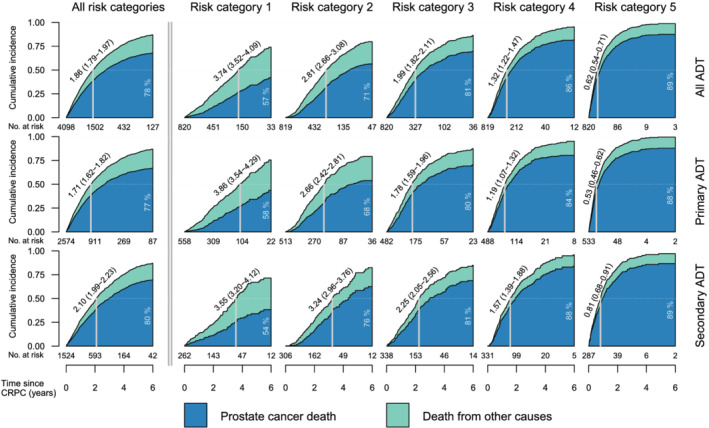
Results: PSA-DT and PSA at date of CRPC are the strongest variables associated with PC specific survival. At the end of follow-up, the proportion of men who died due to PC was 57%, 71%, 81%, 86%, and 89% for risk categories one through five, respectively. The median overall survival in our cohort of men with CRPC was 1.86 years (95% CI: 1.79-1.97).
Conclusion: For a man with castration-resistant prostate cancer, there is a high probability that this will be the main cause contributing to his death. However, there is a significant difference in mortality that varies in relation to tumor burden assessed as PSA doubling time and PSA at time of CRCP. This information could be used in a clinical setting when deciding when to treat more or less aggressively once entering the CRPC phase of the disease.
Keywords: PSA at time of CRPC; PSA doubling time; castration resistant prostate cancer; mortality; mortality in castration resistant prostate cancer; natural history cohort; real‐world cohort.
© 2021 The Authors. BJUI Compass published by John Wiley & Sons Ltd on behalf of BJU International Company.
Figures
References
-
- Petrylak DP, Tangen CM, Hussain MHA, Lara PN Jr, Jones JA, Taplin ME, et al. Docetaxel and estramustine compared with mitoxantrone and prednisone for advanced refractory prostate cancer. N Engl J Med. 2004;351(15):1513–20. - PubMed
-
- Tannock IF, de Wit R, Berry WR, Horti J, Pluzanska A, Chi KN, et al. Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer. N Engl J Med. 2004. Oct 7;351(15):1502–12. - PubMed
-
- James ND, Sydes MR, Clarke NW, Mason MD, Dearnaley DP, Spears MR, et al. Addition of docetaxel, zoledronic acid, or both to first‐line long‐term hormone therapy in prostate cancer (STAMPEDE): Survival results from an adaptive, multiarm, multistage, platform randomised controlled trial. Lancet. 2016;387:1163–77. - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous