

Clinical Relevance of Ischemia with Nonobstructive Coronary Arteries According to Coronary Microvascular Dysfunction
- PMID: 35475358
- PMCID: PMC9238617
- DOI: 10.1161/JAHA.121.025171
Clinical Relevance of Ischemia with Nonobstructive Coronary Arteries According to Coronary Microvascular Dysfunction
Abstract
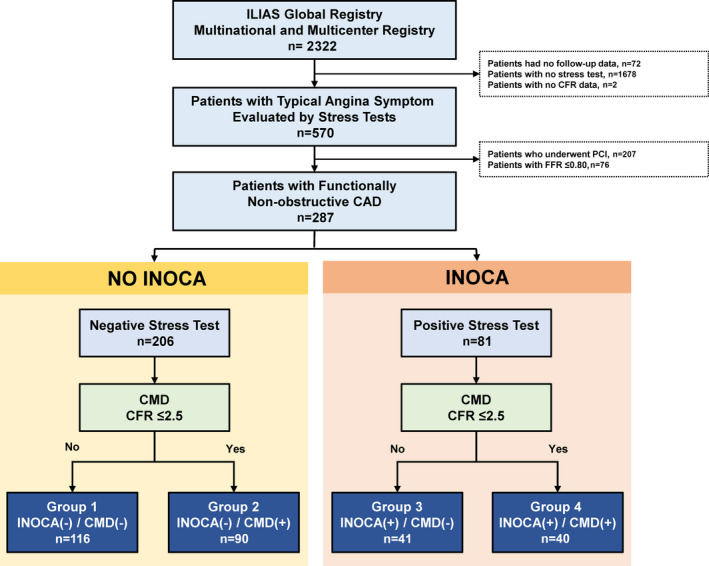
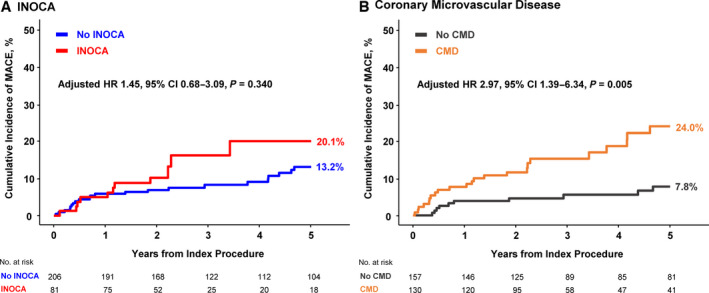
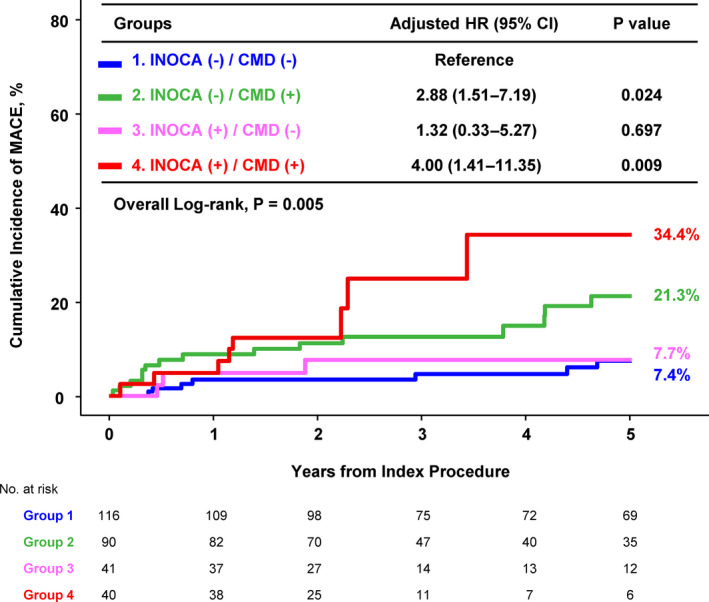
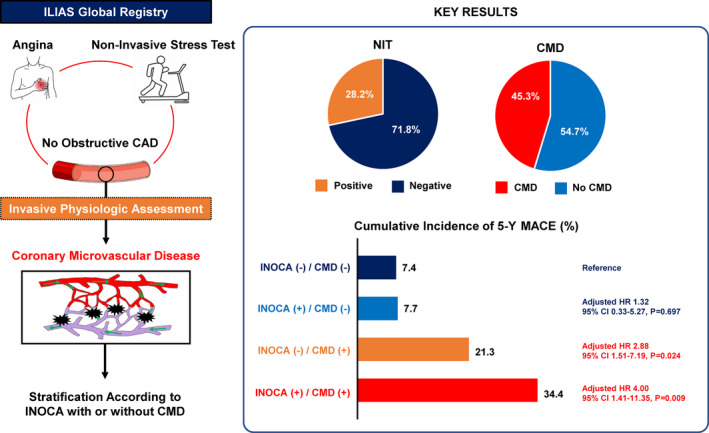
Background In the absence of obstructive coronary stenoses, abnormality of noninvasive stress tests (NIT) in patients with chronic coronary syndromes may indicate myocardial ischemia of nonobstructive coronary arteries (INOCA). The differential prognosis of INOCA according to the presence of coronary microvascular dysfunction (CMD) and incremental prognostic value of CMD with intracoronary physiologic assessment on top of NIT information remains unknown. Methods and Results From the international multicenter registry of intracoronary physiologic assessment (ILIAS [Inclusive Invasive Physiological Assessment in Angina Syndromes] registry, N=2322), stable patients with NIT and nonobstructive coronary stenoses with fractional flow reserve >0.80 were selected. INOCA was diagnosed when patients showed positive NIT results. CMD was defined as coronary flow reserve ≤2.5. According to the presence of INOCA and CMD, patients were classified into 4 groups: group 1 (no INOCA nor CMD, n=116); group 2 (only CMD, n=90); group 3 (only INOCA, n=41); and group 4 (both INOCA and CMD, n=40). The primary outcome was major adverse cardiovascular events, a composite of all-cause death, target vessel myocardial infarction, or clinically driven target vessel revascularization at 5 years. Among 287 patients with nonobstructive coronary stenoses (fractional flow reserve=0.91±0.06), 81 patients (38.2%) were diagnosed with INOCA based on positive NIT. By intracoronary physiologic assessment, 130 patients (45.3%) had CMD. Regardless of the presence of INOCA, patients with CMD showed a significantly lower coronary flow reserve and higher hyperemic microvascular resistance compared with patients without CMD (P<0.001 for all). The cumulative incidence of major adverse cardiovascular events at 5 years were 7.4%, 21.3%, 7.7%, and 34.4% in groups 1 to 4. By documenting CMD (groups 2 and 4), intracoronary physiologic assessment identified patients at a significantly higher risk of major adverse cardiovascular events at 5 years compared with group 1 (group 2: adjusted hazard ratio [HRadjusted], 2.88; 95% CI, 1.52-7.19; P=0.024; group 4: HRadjusted, 4.00; 95% CI, 1.41-11.35; P=0.009). Conclusions In stable patients with nonobstructive coronary stenoses, a diagnosis of INOCA based only on abnormal NIT did not identify patients with higher risk of long-term cardiovascular events. Incorporating intracoronary physiologic assessment to NIT information in patients with nonobstructive disease allowed identification of patient subgroups with up to 4-fold difference in long-term cardiovascular events. Registration URL: https://www.clinicaltrials.gov; Unique identifier: NCT04485234.
Keywords: coronary flow reserve; coronary microvascular disease; ischemia with nonobstructive coronary arteries; myocardial ischemia; prognosis.
Figures
References
-
- Jespersen L, Hvelplund A, Abildstrom SZ, Pedersen F, Galatius S, Madsen JK, Jorgensen E, Kelbaek H, Prescott E. Stable angina pectoris with no obstructive coronary artery disease is associated with increased risks of major adverse cardiovascular events. Eur Heart J. 2012;33:734–744. doi: 10.1093/eurheartj/ehr331 - DOI - PubMed
-
- Reynolds HR, Picard MH, Spertus JA, Peteiro J, Lopez Sendon JL, Senior R, El‐Hajjar MC, Celutkiene J, Shapiro MD, Pellikka PA, et al. Natural history of patients with ischemia and no obstructive coronary artery disease: the CIAO‐ISCHEMIA study. Circulation. 2021. doi: 10.1161/CIRCULATIONAHA.120.046791 - DOI - PMC - PubMed
-
- Bairey Merz CN, Pepine CJ, Walsh MN, Fleg JL, Camici PG, Chilian WM, Clayton JA, Cooper LS, Crea F, Di Carli M, et al. Ischemia and no obstructive coronary artery disease (INOCA): developing evidence‐based therapies and research agenda for the next decade. Circulation. 2017;135:1075–1092. doi: 10.1161/circulationaha.116.024534 - DOI - PMC - PubMed
-
- Shimokawa H, Suda A, Takahashi J, Berry C, Camici PG, Crea F, Escaned J, Ford T, Yii E, Kaski JC, et al. Clinical characteristics and prognosis of patients with microvascular angina: an international and prospective cohort study by the Coronary Vasomotor Disorders International Study (COVADIS) Group. Eur Heart J. 2021. doi: 10.1093/eurheartj/ehab282 - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
