

Association of Socioeconomic Status and Infarct Volume With Functional Outcome in Patients With Ischemic Stroke
- PMID: 35476065
- PMCID: PMC9047646
- DOI: 10.1001/jamanetworkopen.2022.9178
Association of Socioeconomic Status and Infarct Volume With Functional Outcome in Patients With Ischemic Stroke
Abstract
Importance: Long-term disability after stroke is associated with socioeconomic status (SES). However, the reasons for such disparities in outcomes remain unclear.
Objective: To assess whether lower SES is associated with larger admission infarct volume and whether initial infarct volume accounts for the association between SES and long-term disability.
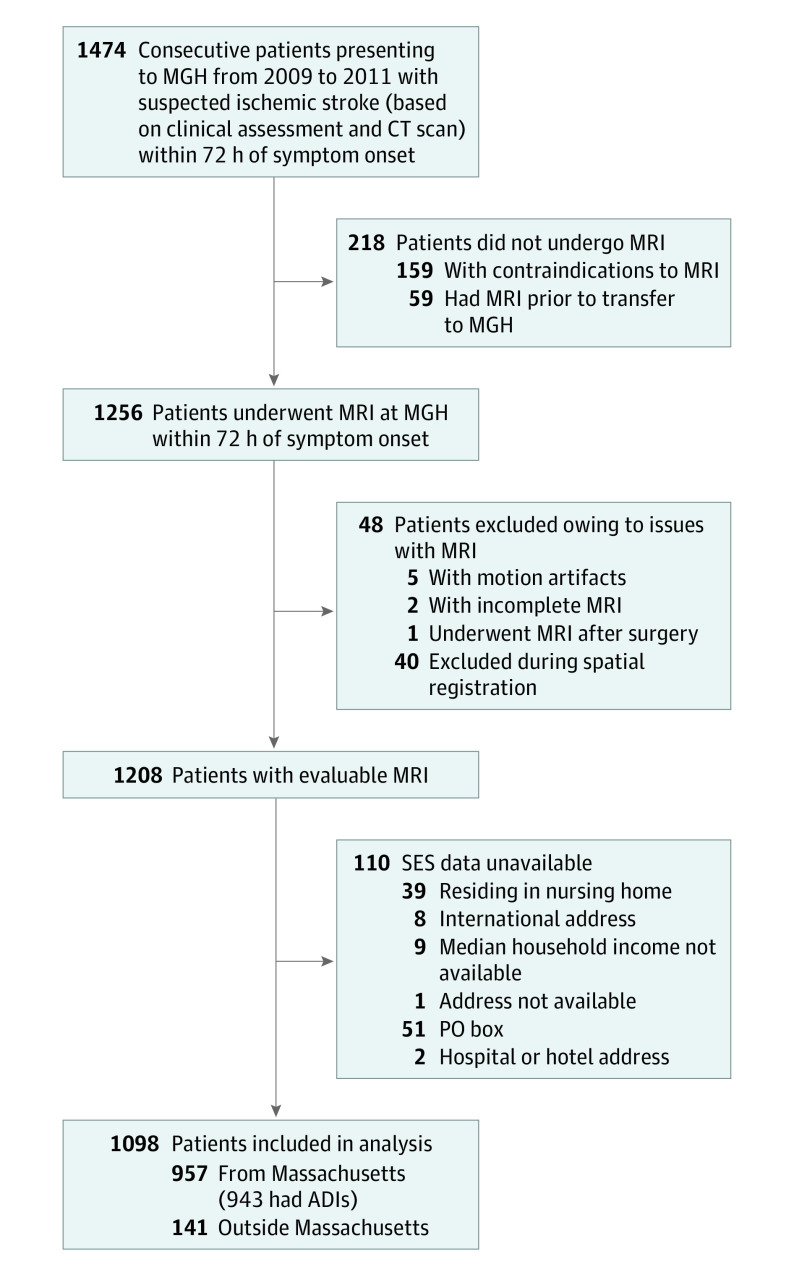
Design, setting, and participants: This cohort study was conducted in a prospective, consecutive population (n = 1256) presenting with acute ischemic stroke who underwent magnetic resonance imaging (MRI) within 24 hours of admission. Patients were recruited in Massachusetts General Hospital, Boston, from May 31, 2009, to December 31, 2011. Data were analyzed from May 1, 2019, until June 30, 2020.
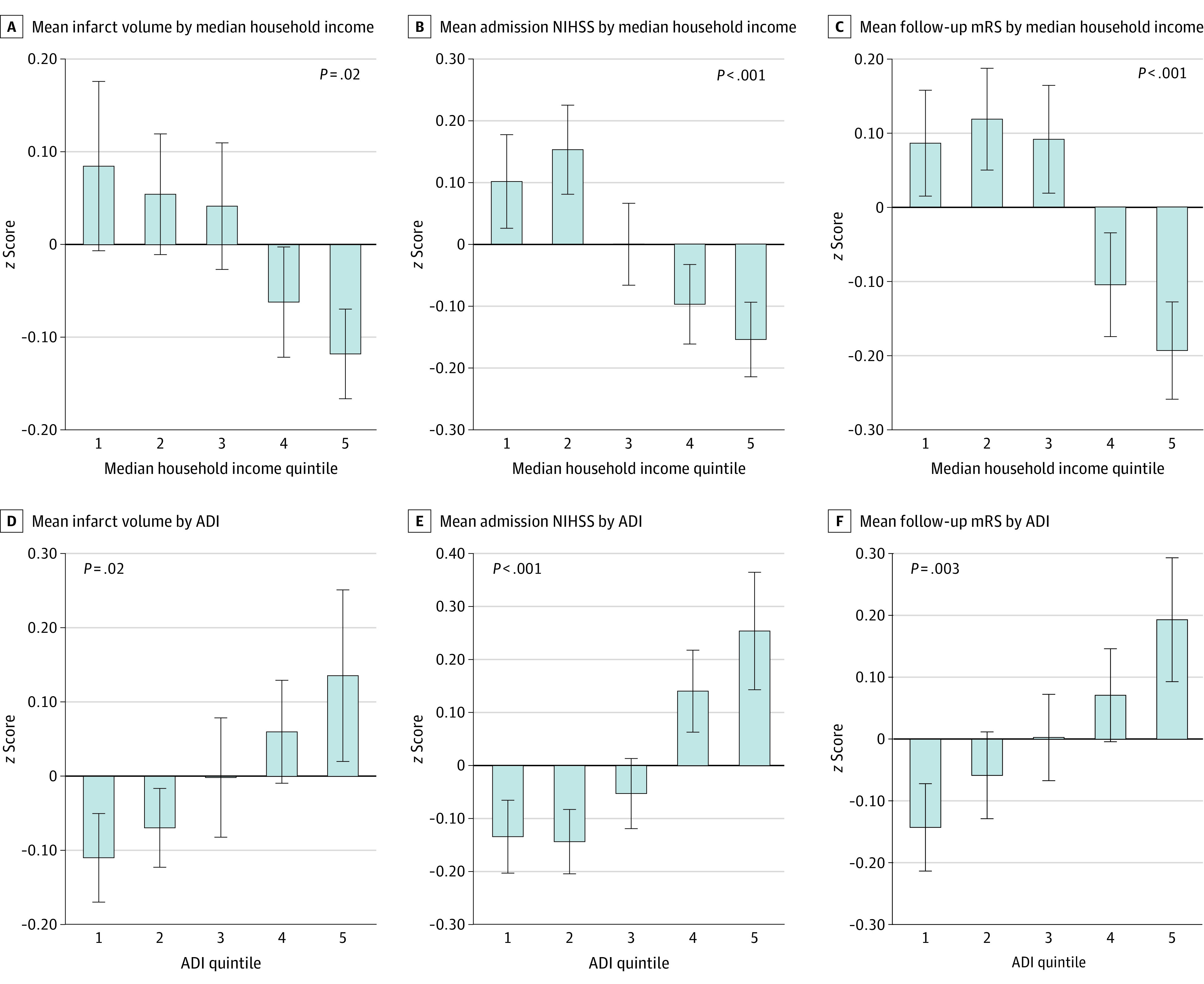
Main outcomes and measures: Initial stroke severity (within 24 hours of presentation) was determined using clinical (National Institutes of Health Stroke Scale [NIHSS]) and imaging (infarct volume by diffusion-weighted MRI) measures. Stroke etiologic subtypes were determined using the Causative Classification of Ischemic Stroke algorithm. Long-term stroke disability was measured using the modified Rankin Scale. Socioeconomic status was estimated using zip code-derived median household income and census block group-derived area deprivation index (ADI). Regression and mediation analyses were performed.
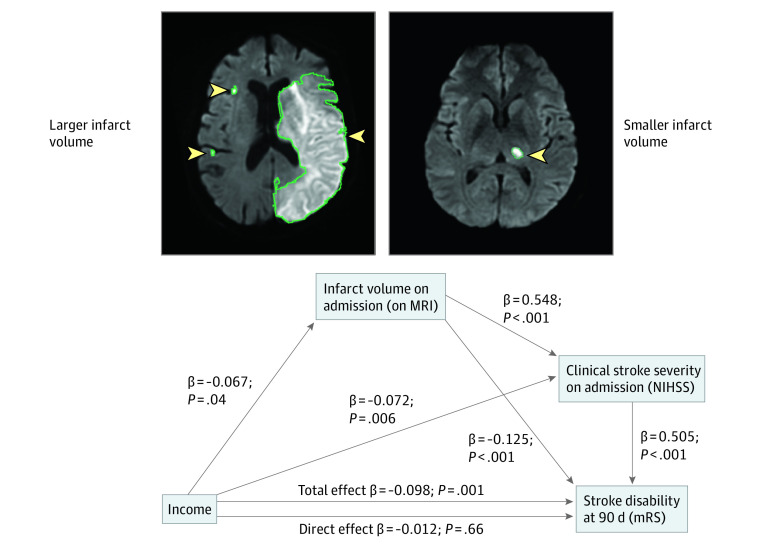
Results: A total of 1098 patients had imaging and SES data available (mean [SD] age, 68.1 [15.7] years; 607 men [55.3%]). Income was inversely associated with initial infarct volume (standardized β, -0.074 [95% CI, -0.127 to -0.020]; P = .007), initial NIHSS (standardized β, -0.113 [95% CI, -0.171 to -0.054]; P < .001), and long-term disability (standardized β, -0.092 [95% CI, -0.149 to -0.035]; P = .001), which remained significant after multivariable adjustments. Initial stroke severity accounted for 64% of the association between SES and long-term disability (standardized β, -0.063 [95% CI, -0.095 to -0.029]; P < .05). Findings were similar when SES was alternatively assessed using ADI.
Conclusions and relevance: The findings of this cohort study suggest that lower SES is associated with larger infarct volumes on presentation. These SES-associated differences in initial stroke severity accounted for most of the subsequent disparities in long-term disability in this study. These findings shift the culpability for SES-associated disparities in poststroke disability from poststroke factors to those that precede presentation.
Conflict of interest statement
Figures
References
-
- Heron M. Deaths: leading causes for 2016. Natl Vital Stat Rep. 2018;67(6):1-77. - PubMed
-
- Benjamin EJ, Virani SS, Callaway CW, et al. ; American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee . Heart disease and stroke statistics—2018 update: a report from the American Heart Association. Circulation. 2018;137(12):e67-e492. doi:10.1161/CIR.0000000000000558 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
