

Multiple sclerosis: Immunopathological heterogeneity and its implications
- PMID: 35476319
- PMCID: PMC9324211
- DOI: 10.1002/eji.202149757
Multiple sclerosis: Immunopathological heterogeneity and its implications
Abstract
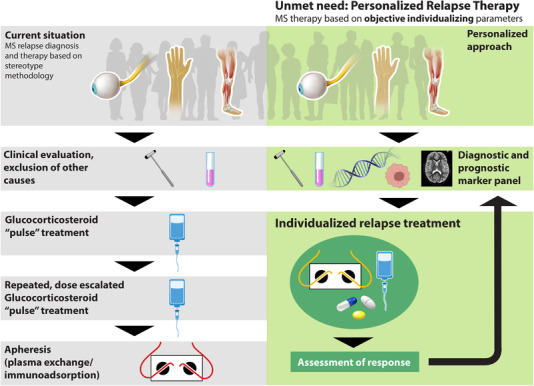
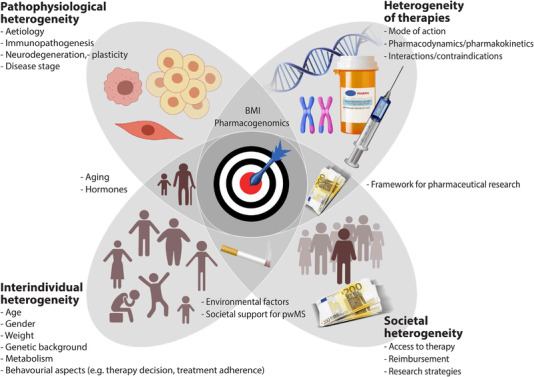
MS is the most common autoimmune demyelinating disease of the CNS. For the past decades, several immunomodulatory disease-modifying treatments with multiple presumed mechanisms of action have been developed, but MS remains an incurable disease. Whereas high efficacy, at least in early disease, corroborates underlying immunopathophysiology, there is profound heterogeneity in clinical presentation as well as immunophenotypes that may also vary over time. In addition, functional plasticity in the immune system as well as in the inflamed CNS further contributes to disease heterogeneity. In this review, we will highlight immune-pathophysiological and associated clinical heterogeneity that may have an implication for more precise immunomodulatory therapeutic strategies in MS.
Keywords: precision medicine ⋅ biomarkers ⋅ brain barriers immunotherapy ⋅multiple sclerosis.
© 2022 The Authors. European Journal of Immunology published by Wiley-VCH GmbH.
Conflict of interest statement
BE received a grant from Biogen to study extended dosing of Natalizumab on T‐cell migration across the blood–brain barrier and a grant from CSL Behring to investigate the molecular underpinnings of blood brain barrier dysfunction in neurological disorders. BE is a co‐inventor on provisional US patent applications related to the EECM‐BMEC‐like cells (63/084980 and 63/185815). MC reports no conflict of interest in relation with this publication. AC has received speakers’/board honoraria from Actelion (Janssen/J&J), Almirall, Bayer, Biogen, Celgene (BMS), Genzyme, Merck KGaA (Darmstadt, Germany), Novartis, Roche, and Teva, all for hospital research funds and not related to this publication. He received research support from Biogen, Genzyme, and UCB, the European Union, and the Swiss National Foundation (SNF no. 310030_172952).
Figures
References
-
- Thompson, A.J. , Banwell, B.L. , Barkhof, F. , Carroll, W.M. , Coetzee, T. , Comi, G. , Correale, J. et al., Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018. 17: 162–173. - PubMed
-
- Baecher‐Allan, C. , Kaskow, B.J. and Weiner, H.L. , Multiple sclerosis: mechanisms and immunotherapy. Neuron 2018. 97: 742–768. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
