

Stage Shift as an Endpoint in Cancer Screening Trials: Implications for Evaluating Multicancer Early Detection Tests
- PMID: 35477176
- PMCID: PMC9250620
- DOI: 10.1158/1055-9965.EPI-22-0024
Stage Shift as an Endpoint in Cancer Screening Trials: Implications for Evaluating Multicancer Early Detection Tests
Abstract
Background: Disease-specific mortality is a consensus endpoint in cancer screening trials. New liquid biopsy-based screening tests, including multi-cancer early detection (MCED) tests, are creating a need to reduce the typically lengthy screening trial process. Endpoints based on the reduction in late-stage disease (stage shift) have been proposed but it is unclear how well they predict the impact of screening on disease-specific mortality across a variety of cancers potentially detectable by MCED tests.
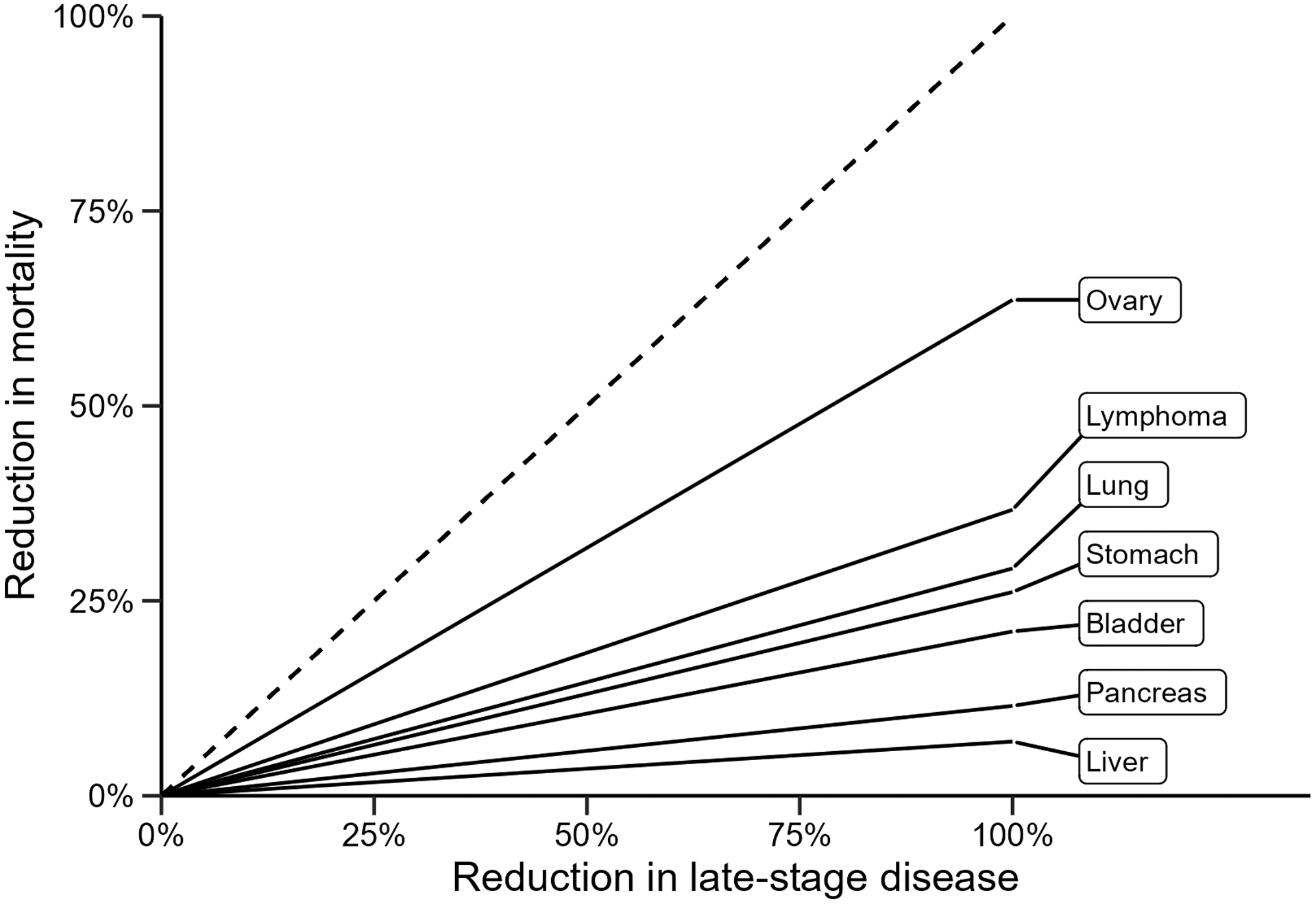
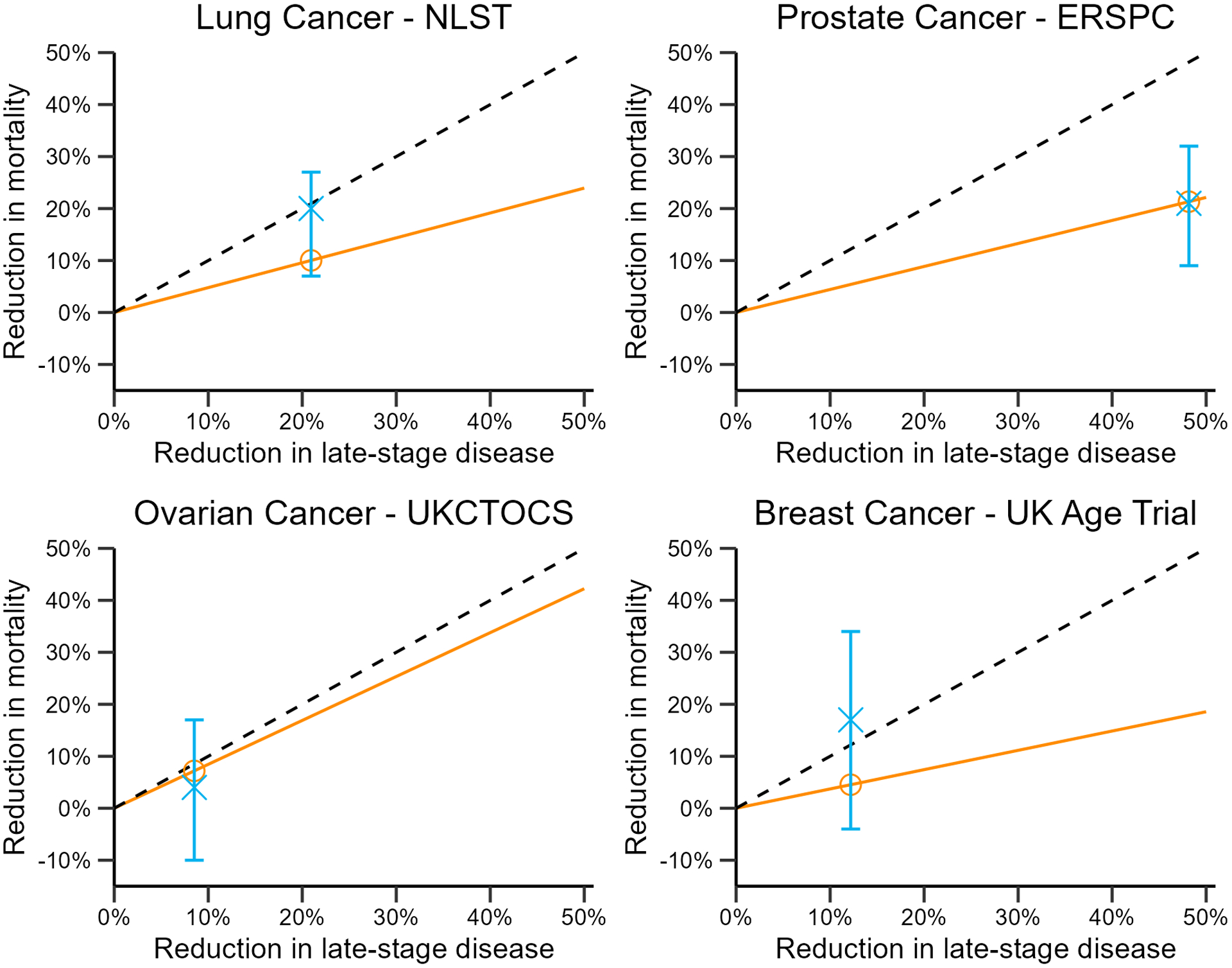
Methods: We develop a mathematical formulation relating the reduction in late-stage cancer to the expected reduction in disease-specific mortality if cases diagnosed early via screening receive a corresponding shift in mortality. We investigate the similarity between the expected mortality reduction and the observed mortality reduction in published trials of screening for breast, lung, ovarian, and prostate cancer.
Results: The expected mortality reduction for a given stage shift varies significantly depending on cancer- and stage-specific survival distributions, with some cancer types showing little possibility for mortality improvement even under substantial stage shift. The expected mortality reduction fails to consistently match the mortality outcomes of published trials.
Conclusions: In MCED, any mortality benefit is likely to vary substantially across target cancers. Stage shift does not appear to be a reliable basis for inference about mortality reduction across cancers potentially detectable by MCED tests.
Impact: Stage shift may be an appealing endpoint for evaluation of cancer screening tests but it appears to be an unreliable predictor of mortality benefit; furthermore, the same stage shift can mean different things for different cancers.
©2022 American Association for Cancer Research.
Conflict of interest statement
Figures
References
-
- Connor RJ, Chu KC, and Smart CR. “Stage-shift cancer screening model”. J Clin Epidemiol 1989; 42.11:1083–1095. - PubMed
-
- Feuer EJ, Mariotto A, Merrill A. “Modeling the impact of the decline in distant stage disease on prostate carcinoma mortality rates”. Cancer 2002; 95.4: 870–880. - PubMed
-
- Clarke CA, Hubbell E, Kurian AW, Colditz GA, Hartman A, Gomez SL. “Projected Reductions in Absolute Cancer-Related Deaths from Diagnosing Cancers Before Metastasis, 2006–2015”. Cancer Epidemiol. Biomark. Prev 2020; 29.5: 895–902. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
